Diseases
Migraine / Headaches
Disease
Migraine Headache
Are you suffering from headaches? You are not alone! Headache is a widespread disease and one of the most common reasons to visit a Neurologist in Dubai. It occurs in different types and strengths and can impair the quality of living substantially. It is possible to do something against it. But before a therapy can be started it has to be found out what the reason is and a correct diagnosis has to be made.
Types of headaches
There are many types of headaches. The most common are the primary headaches like migraine, tension headache or cluster headache or an analgetic headache. Your neurologist has to know how your headache feels like, where it starts; whether there are accompanying symptoms, how long it lasts and how often it occurs. Then he will do different medical examinations. After he knows the diagnosis he can give you an advice for the right treatment. Treatment is possible!
Migraine
Migraine is one of the most frequent neurological diseases. Around the world about 10 percent of the adults are suffering of migraine, more women than men. The difference between the genders has most likely hormonal and genetic reasons, neurologists assume. Typically it starts in adolescence. After the 50th year the frequency declines again.
The duration of a pain attack is between 4 to 72 hours. The frequency varies between once a year up to twice a week. The pain is moderate up to very violent. The characteristic is mostly pulsating and only on one side of the skull; but in some patients also on both sides. One side is more affected than the other. Very often people are having accompanying symptoms like nausea, vomiting, visual problems and are very sensitive against light, noise and odour. By physical exercises the pain increases.
A typical migraine attack proceeds in 4 phases. During the lead time there exist no pains yet. There could be depressive reactions, irritability and agitation. It’s important to report also sensations like these to your neurologist; even if you think it has nothing to do with the pain itself. Concentration might get reduced; people feel tired and have to yawn a lot. Oedema, constipation or a craving for sweet or greasy food may occur. The second phase might be an aura. Quite often there are visual problems with scintillating scotomas or double vision. But it also can be sensibility disturbances or movement and speech problems. An aura keeps from a few minutes up to one hour.
The third phase neurologists call the headache phase. The pulsating pain starts very often in the neck, spreads over the back of the head and settles behind the eye or at the temple. Most attacks are accompanied by vegetative symptoms. The whole body is affected. Some people are not able to continue their work. They have to lie down. They seek quietness and darkness, don`t want to hear or see anything or anybody. The duration of the headache might be up to 3 days if the attack is not interrupted by medication. Hours or 1-2 days after a migraine attack (4th phase) people feel tired and exhausted, concentration is still reduced, mood might be swinging.
Causes
It is a temporary dysfunction of the brain. During a migraine attack the blood vessels of the cerebral membrane are widened and inflamed. The nerve fibres around the vessels are irritated so heavily that they send pain signals.
There are different migraine triggers like stress, menstruation, alcohol, especially red wine, disturbances in the sleep-awake-cycle, irregular meals, weather changes, light stimulus, odour or pain in the neck. These triggers are very individual and vary even in one individual from time to time. But these triggers are not the causes of the disease they just stimulate it.
Treatment
Nowadays neurologists are using very effective and fast treatment options for migraine headaches.
If you think that visiting a neurologist might not fix what you're going through. GNC Dubai is providing one of the best psychiatrists in Dubai, psychologists in Dubai and psychotherapists in Dubai who can help you find the core reason and in fixing it.
Migraine treatment without medication:
1. Reduce stress factors as much as possible
- Learn good time management: plan your day schedule. Don`t forget enough time for brakes.
- Learn to say “No”.
- Don`t spread yourself too thin. Not everything has to be done right away.
- Think: “nobody is perfect!”
- Take life easier, enjoy it.
2. Relaxation
Proceedings for recreation as Yoga, autogenic training or progressive muscle relaxation techniques help, but have to be done regularly
3. Psychotherapy
Research could show that Cognitive Behavioral Therapy (CBT) has a positive impact on migraine patients. Even consulting a patient is able to reduce the frequency of migraine attacks. Therefore CBT was included in the Guidelines of the German Headache and Migraine Association.
4. Endurance sports
Endurance sports like cycling, walking, jogging or swimming are good. But it is important to exercise regularly, at least three times a week for about 30 minutes.
5. Sleep
Constant sleep-awake cycle, also during the weekend. And eat and drink with regularity.
6. Triggers
Avoid your personnel migraine triggers.
Migraine treatment with medication
1. Therapy of the acute migraine attacks
There are different types of medication to treat the acute attack. In easier cases common painkillers can be enough. A combination with a medication against nausea can be given. But mostly stronger medication is required. Special migraine drugs can ameliorate the attack within 2 hours in most patients. This kind of medication needs to be prescribed by a neurologist. The medication has to be taken as soon as possible. Then it helps the best. But be careful. You should not take any painkiller more often than 10-12 times a month. Otherwise there is the danger to develop an analgesic headache, which means headache by the medication itself!
2. Migraine Medical prophylaxis
In severe cases it is useful to take special medication every day to reduce the number of attacks, the length of the single attack or to improve the effect of the acute medication. This medication has to be taken for at least three quarters of a year, sometimes longer. Your neurologist will find out which medication will be the best for you and will supervise you through the therapy.
© GNC, German Neuroscience Center Dubai (Neurology, Psychiatry, Psychology, Counseling, Dubai, UAE)
Vertigo
Disease
Vertigo, Dizziness, Giddiness, Lightheadedness
Approximately 15% of the population is suffering from dizziness, vertigo, imbalance, lightheadedness, giddiness or unsteadiness. Vertigo is the perception of movement without actual movement (illusion of motion). Most commonly it is the sensation of spinning (either the room spinning or the person spinning). But it can be the sensation lateral movement, swaying or tilting, too. Vertigo is a type of dizziness. However, dizziness could also include other symptoms which not necessarily come with the feeling of spinning, such as imbalance, lightheadedness, giddiness and unsteadiness. Vertigo is a symptom, not a diagnosis. Meaning that vertigo can be caused by a wide range of diseases; from harmless to life threatening. In this article we focus on the most common neurological diseases.
Symptoms & Signs
Most commonly patients will experience the feeling of dizziness, vertigo, imbalance, lightheadedness, giddiness or unsteadiness. Moreover postural instability and feeling of falling or actual falling. Patients often need to sit or lie down and are suffering from nausea or vomiting. Ataxia (walking difficulties) and nystagmus (eye movements) could be present. Depending on the underlying cause the following symptoms could be present: hearing loss, tinnitus, ear pressure, visual problems. Moreover numbness of the skin, muscular weakness, coordination problems, speech or language difficulties, difficulty swallowing.

Causes
The causes of vertigo or dizziness can be manifold. There are various diseases that could cause the symptom of vertigo. It can be a disease of the ear or inner ear, the vestibular nerve or the brainstem. It could take comprehensive examinations to find out the real cause. Here we would like to highlight the most common causes.
1. Benign paroxysmal positional vertigo (BPPV): Benign paroxysmal positional vertigo is the most common cause of vertigo. Certain head movements can provoke a vertigo attack. The attacks are short (<30sec). Often the vertigo attack occurs in the night while rolling over in bed. This from of vertigo is caused by small crystals of calcium deposits in the ear canal that periodically become dislodged by specific head positions or movements. It is a very common form of vertigo.
2. Vestibular neuritis: Vestibular Neuritis is caused by an inflammation of the nerve to the semicircular canals, which helps control the balance. It is characterized by a sudden severe attack of vertigo, which lasts for seven to ten days.
3. Ménière disease: This disorder of the inner ear causes spontaneous episodes of vertigo along with fluctuating hearing loss. It is often attended by a Tinnitus (ringing in the ear) and a feeling of pressure or fullness in the ear.
5. Labyrinthitis: An inflammation of the inner ear structure called the labyrinth, caused by untreated bacterial infections of the middle ear. It can also cause loss of hearing.
6. Head trauma: A violent blow on the head can cause damage to the inner ear. This may lead to balance problems like Vertigo or Dizziness, temporary or permanent.
7. Others: Migraine, Superior canal dehiscence syndrome, Otitis media, Herpes zoster oticus, heart diseases and low blood pressure, Parkinson disease, Brain Stroke, Brain tumor, Acoustic neurome, Vestibular schwannoma, Epilepsy, Chiari malformation, Multiple sclerosis, Cholesteatom, Perilymphatic fistula, Superior semicircular canal dehiscence syndrome, Autoimmune disease, Psychological disorders like panic attacks or anxiety
Diagnostic procedures
First step should always be a consultation (important is the onset, triggers, duration, frequency, accompanying symptoms of the vertigo) and a comprehensive neurological examination (including coordination, nystagmus and gait testing). Only then a experienced neurologist can evaluate which further tests could be necessary. Such as Dix-Hallpike test, AEP, auditory evoked potentials, Vestibular evoked myogenic potentials, audiogram (hearing test), Tympanometry, Videonystagmography, Electrocochleography, Computed tomography (CT) or MRI
Treatment
The treatment of vertigo depends on the underlying cause. Only if the neurologist could find out the cause by the above mentioned procedures the treatment should start. If the cause is life threatening like an acute stroke immediate action has to be taken. Most commonly the treatment is not that urgent. In the following we give you a short overview of possible treatment options. However, which ones apply depends on the findings I the diagnostics.
1. Repositioning maneuvers for BPPV (eg Epley maneuver or Semont maneuver)
2. Pharmacotherapy: Vestibular suppressants (Meclizine, benzodiazepines), corticosteroids and diuretics, β-blockers, calcium-channel blockers, antidepressants, anticonvulsants.
3. Physical Exercise or physical therapy Generally speaking physical activity is positive because the inner ear gets trained by this. Dangerous situations or the risk of falling should be avoided of course.
4. Lifestyle: In case of migraine vertigo trigger situation should be avoided. Further migraine treatment cou can find here.
Professor Dr. med. Detlef Koempf – Neurologist & Expert for Vertigo & Visual Problems

Professor Koempf, Specialist for vertigo & visual Problems, is a genuine German University Professor born in Saeckingen, near Freiburg and studied medicine in Heidelberg.
After having spent one year of research in the USA, he continued his medical education at the University Hospitals Mannheim and Heidelberg and went on to work as Deputy Head at the Neurological Hospital in Erlangen.From 1987 until 2010, Professor Koempf held the position as Director of the Neurological University Hospital of Luebeck, Germany where he worked as a Senior Consultant for Neurology, held lectures and taught students. In 2010 he was elected as General Secretary to the EFNS (European Federation of Neurological Societies) where he organizes large neurological conventions and further education for neurologists in Eastern Countries such as Russia, Belarus, Ukraine, Moldavia and others.
Aim of these efforts is to standardize neurological diagnostics and treatment in Europe.In 1998, Professor Koempf wrote an important book on the topic of “Clinical Neuro-Ophthalmology”, vertigo and visual problems which was published by the renowned Thieme Publishers. He also deals with all “Diseases of the Cranial Nerves” on which he also published a book in 2006.Since finishing his Univerity career, Professor Koempf has been seeing patients in his private clinic in Luebeck and spends some months in Mallorca, Spain, in a Vertigo Center which he founded at Juaneda Hospital.
During his active time as Director of the Neurological Hospital at Luebeck University, Professor Koempf dealt with the whole range of neurological diseases including Parkinson’s disease, Epilepsy, Multiple Sclerosis, Cerebral circulatory disorders, stroke prophylaxis, disturbances of the memory, dementia, headaches, migraine, polyneuropathies, restles legs syndrome, back pain and diseases if the discs.But above all, he concentrated on the numerous kinds of vertigo (of which there are about 50) as well as vision disorders or disturbances of the equilibrium. Vertigo itself is just a very general term which does not mean anything specific. One must differentiate between specific vertigo meaning everything is spinning and unspecific vertigo which may mean short loss of vision, dizziness or disturbed equilibrium.The problem always is to find the underlying cause because very often the cause of very strong symptoms may be quite harmless whereas a slight symptomatology may indeed have a dangerous cause. In the latter case, a fast course of diagnostics is of the utmost importance in order to prevent for instance a stroke. The whole range vertigo lies between these two poles.The most important issue when dealing with vertigo symptoms is the medical history and the correct analysis of the symptoms. At the beginning of this procedure there will be a thorough neurological examination with a focus on the eye movements.
From time to time it will be necessary to carry out a psychiatric exploration as well because vertigo can be due to psychic problems. Following this will be neurophysiological investigations such as EEG, VEP, AEP or others and the DUPLEX ultrasound examination of the cranial arteries and a combined cooperation with an ENT doctor, an ophthalmologist, maybe an orthopedist and a qualified laboratory. Despite his being in Dubai only recently, Professor Koempf realized that all services he needs for his highly specialized work are available in Dubai, predominantly offered by German colleagues such as ophthalmology, ENT, orthopedics, cardiology and laboratory. This makes diagnostics and treatment easier since they all follow the same high German standards and uncomplicated communication between them allows secured results. Professor Koempf is devoting some of his time at the moment to meeting and getting to know these colleagues in order to guarantee best results for his patients. As main problems in this region, Professor Koempf notices so far the often faulty medicinal treatment of patients suffering from Parkinson’s disease or epilepsy, missing preventative measures for stroke and other diseases of the vessels as well as pain therapy regarding the numerous kinds of headaches or polyneuropathy caused by diabetes. Above all he is concerned about people suffering from dizziness and vertigo which is one of the most prevalent complaints presented in a neurological clinic and not to be underestimated regarding the possibly underlying serious causes.Professor Koempf will continue to inform us about the topic of vertigo on this site.
We can also help you with the best psychologist, psychiatrist and psychotherapist available in Dubai, UAE.
Book Your Appointment with Prof Koempf - Vertigo Expert
Saturday - Wednesday: 9am to 8pm Thursday: 9am - 7pm JLT Jumeirah Lake Towers, Cluster I, Platinum Tower 2806 Right side: 3hrs free parking Left side: all day free parking DHCC Dubai Healthcare City, Bld.
© GNC, German Neuroscience Center Dubai (Neurology, Psychiatry, Psychology, Counseling, Dubai, UAE)
Sciatica
Sciatica
Sciatica is a common neurological condition described as pain, numbness, weakness, or tingling radiating from the lower back to the leg. The symptoms usually occur on one side and vary from mild to unbearable.
It is important to understand that sciatica is not a disease itself. It is rather a symptom caused by an underlying condition. In most cases the underlying condition is a herniated disc, other degenerative disc diseases or spinal stenosis.
The treatment depends on the underlying conditions. Usually Sciatica has a very good prognosis if the treatment is started early enough.
Causes
Sciatica can be caused by any underlying condition that squeezed the sciatic nerve. The sciatic nerve is a large nerve that starts in the lower back and runs down the back of each leg. It controls the muscles and the sensation of the leg and foot.
Read MoreConditions that may cause sciatica
• Bulging or herniated disk in the back (most common)
• Other degenerative disk disorders
• Lumbar spinal stenosis
• Piriformis syndrome
• Tumor and others

Signs & Symptoms
The symptoms are depending on anatomical structure and the function of the sciatic nerve (see above). The following symptoms may occur in the lower back, the buttock, the hip and the leg:
Read More• Pain: Often the pain is described as a sharp pain. The pain can be so severe that movements may be difficult.
• Tingling, burning, numbness or other sensory symptoms
• Weakness of the muscles and problems to move the leg
Symptoms may worsen when you cough, sneeze, or laugh, or when you sit or stand for long periods of time. Being overweight is a risk factor.
Treatment
As a first step, it is important to find the underlying condition causing the sciatica. A neurologist can find the location of the lesion by the symptoms presented. Depending on the location (L4, L5, S1) symptoms in the leg may vary. The treatment depends on the underlying condition and the severity of symptoms. If the symptoms are very mild and there is no danger of worsening, the symptoms may improve on its own.
Depending on the underlying condition the treatment may include:
Read More• Medication: Most patients need pain relieving medication. Moreover, medication that relaxes the muscles and thus reduces the pressure on the nerve may help as well.
• Physiotherapy: Initially it is important to reduce any movement that puts pressure on the sciatic nerve. Moreover, strengthening and stretching exercises may applicable. Applying heat or icing brings relief in some patients.
• CBT: Large studies could show that Cognitive behavioral therapy is effective in reducing the pain and coping with the symptoms.
• Injections: In severe cases injections that reduce the pain and inflammation may help.
• Surgery: Surgery should always be the last option and is not required in the vast majority of cases.
Read more about specific treatment of slipped or bulging disk here.
Prognosis
Usually sciatica has a very good prognosis. The sooner the underlying condition is diagnosed and the sooner the correct treatment starts, the better the outcome.
Our Team Of Experts
Since more than ten years GNC is the leading clinic for Neurology in the UAE. All our Sciatica experts are German Board Certified and have minimum professional experience of 25 years. If you are searching for the most trusted Sciatica experts, you came to the right place.
Testimonials
``The doctor is the best and everyone's very helpful``
``Excellent doctor``
``I am thankful for the service.``
``Being able to have blood tests and EEG done at the clinic itself was very helpful and convenient. This also allowed my doctor to have fast access to the test results.``
``I'm impressed by the Professor and team professionalism``
``God bless you guys wish you more of success``
``Great service``
``It was a great visit thanks! It really helped me.``
As Seen On


Back Pain Treatment in Dubai
Back pain is among the most common medical problem in modern society and one of the most common conditions treated by our experts. Up to 84 percent of adults experience back pain at some time in their lives. Back pain could occur at all ages with a peak around 40-50. Back pain is worldwide the most common cause of disability in persons younger than 40. Back Pain can have many different causes. Therefore, as a first step, it is important to find the underlying cause and plan the right treatment according to it. Most causes of back pain are treatable with good results and surgery can be avoided. Moreover, there are very effective measures to prevent back pain from reoccurring.Types of Back Pain
Acute vs chronic back pain: Acute back pain is most often caused by an injury or wrong movement, has a sudden onset, and lasts only hours our days. Chronic back pain is characterized as a pain lasts more than 12 weeks. Location of pain: Most common is lower or lumbar pain, but the pain can be located in the middle of the back, the upper back or neck, too. In disc related back pain and sciatica we often see a radiating pain down the legs. Severity of pain: from mild to unbearable painSymptoms / Signs
Symptoms could occur after lifting heavy items or other physical exercise. However, it can also occur without any previous activity. Peripheral nerves are having 3 functions: Pain, sensory and motor function. This explains the symptoms.- Back Pain
- Pain in the back, buttock or leg (sciatica)
- sensory loss, numbness or tingling of the skin
- Muscle weakness of the legs
- The pain could lead to muscle strain or spasm of the back muscles. Thus, the movement is impaired and the posture affected.
- A very serious symptom is called cauda equina compression. Neurologists define it as numbness of the legs, bladder / bowel dysfunction and impotence. This requires urgent surgery.
- Neck pain
- Pain in the neck, shoulder, arm, chest, Headache
- Vertigo, dizziness, giddiness, Tinnitus, Visual disturbances
- numbness in arm and hands
- weakness in arm and hands
- The pain could lead to muscle strain or spasm of the back muscles. Thus the movement is impaired and the posture affected.
Causes
Since back pain can be caused by many different underlying conditions, a thorough examination is needed to find the true cause.Some of the most common causes and underlying conditions are:
- Disc diseases
- Osteoarthritis, spondylolisthesis, fractures, osteoporosis, Spinal stenosis, Dysfunction of the joints of the lower back
- Accidents and Muscle strain
- Cancer like bony metastases and others
- Infection like osteomyelitis, tuberculosis, diskitis, epidural abscess and others
- Vascular like abdominal aortic aneurysm, epidural hematoma and others
- Rheumatologically diseases like arthritis and others
Other causes of back pain
- Pain originating in the organs close to the spine, like the stomach, kidneys, or bladder, and can radiate to your back.
- Swelling of the aorta - the main blood vessel going away from the heart - can cause back pain.
- Fibromyalgia - widespread pain and tenderness of the body - can cause back pain.
- Inflammatory diseases, stomach ulcers, and UTIs can hurt your back.
- Women: In the case of women, conditions like pregnancy and fibroids (tumours of the womb) or a disease like endometriosis can cause back pain.
- Men: In the case of men, testicular rupture or testicular torsion can be a cause.
Spondylosis
Ageing can cause our muscles, bones and the discs of the spine to weaken gradually. Everyone goes through this process of weakening of the spine, but that doesn’t necessarily become a cause of pain. The spinal discs are located between the vertebrae (bones making the spine) and act as shock absorbers. As they shrink with time, the space between the vertebrae reduces meanwhile bone spurs start developing along the edges of the vertebrae and joints. In medical terminology, this condition is referred to as spondylosis. As the discs are shrinking, the inner part of the disk, which is still more flexible, breaks thru the outer part and squeezes the nerve roots nearby. Neurologists call this a prolapsed intervertebral disk. Most common locations are the lower back, L4-L5 and L5-S1 or the neck, C5-6 and C6-7.Sciatica
Back pain is often linked to numbness, tingling feeling, or pain in the legs which is a condition called sciatica. It originates when the spinal nerve (sciatic nerve) - running down the back of the legs - gets damaged or squeezed. People with sciatica often feel more intense pain in the legs than in the back or less often feel no pain in the back. A slipped disc or an outgrowth of bone can put pressure on the sciatic nerve and cause pain or numbness along the nerve's pathway. This can cause pain anywhere from the lower back to the foot or toe.Spinal Stenosis
Another condition linked to back pain is spinal stenosis which is characterized by pain in the legs, arms, back, neck, hands, or feet. The pain can start at once and fade away or might get worse over time - depending on the location of the pain. This can be a genetic condition or might be experienced with the growing age. Our spine has a canal that contains the nerves of the spinal cord, the narrowing of this canal can result in spinal stenosis. Some people are born with a narrow canal and some may experience the narrowing of space later in life. Less space can put pressure on the nerves running through this canal, and this results in pain or numbness in different parts. Along with other areas, both or one leg can be affected, and the pain is more severe in the legs than in the back. Some people feel relieved when they sit down or walk while slightly hunching their back.Risk factors
- Obesity
- poor physical health
- poor nutrition
- Smoking
- Heavy manual labor
- Psychological reasons like depression, work related problems and others.
- Pregnancy
- Weather? No! Lower back pain is commonly associated to weather changes. But this seems to be untrue.
Diagnosis
The diagnostic procedures used depend on the patient’s complete medical history and physical examinations which determine if there is any serious underlying condition that could be causing the pain. Only after a thorough back examination and neurological tests can a healthcare provider establish the cause of back pain and the appropriate treatment. A doctor may perform several tests to identify the exact cause of back pain. These tests include;- Consultation
- Physical examination
- Neurological examination
- Electromyography (EMG): checks the electrical activity in the nerves of your spine. It is a minimally invasive technique that helps in identifying the nerve damage causing back pain.
- Nerve Conduction Velocity (NCV) Nerve conduction velocity (NCV) is a diagnostic test that measures the speed at which electrical impulses travel through nerves in the body
- X-rays: This is done to see if there is some sort of dislocation, fracture, or degeneration of bones.
- MRI: An MRI scan is usually performed to get a detailed overview of your spine. This helps in identifying even small changes and problems.
- CT scan: It is helpful in getting a complete and detailed image of your bones. It involves multiple X-rays and helps in diagnosing back pain by providing a 3-D picture of your bones.
When to See a Doctor
Back pain is common and usually gets better within a few days, but there are some conditions when you should see a doctor:- Your pain is getting worse day by day
- If it lasts for more than a week or two
- If you are unable to perform your routine tasks
- You have extreme pain that is interrupting your activities
- You are facing other health problems like fever or difficulty in penile erection
Treatment and prevention
90% of acute back pain cases will fully recover. Patients with subacute or chronic back and neck pain (3 month>) still have a favourable prognosis, however not as positive as acute back pain. Moreover, the treatment of chronic back pain or neck pain differs from treatment of acute pain. There should never be a treatment without a proper examination. Before going into detail, we will answer the most common questions patients will ask:- Do I need to get surgery? Any surgery is a potential harm to the patient. Therefore, there must be a clear indication. Luckily only less than 2% of patients suffering from neck or back pain need surgical intervention.
- Do I need to stay in bed? If the pain is acute, you will most probably lay down anyway. If your muscles cramp and the movement is impaired you don’t have much other possibilities. After the treatment started there is no beneficial effect of prolonged bed rest. Moreover, other problems like thrombosis could occur.
How to Manage Your Back Pain
There are many things you can do to ease your back pain. Staying active and maintaining a healthy lifestyle is a good way to start. Rest is important but preventing your back from any movement can worsen the pain and slow down the recovery process. Mild exercise often speeds up the recovery process. Research also suggests that your emotional responses also play a significant role in speeding up the back pain recovery process. So, one must learn to tackle the emotional challenges to get better faster. If your back pain takes too long to get better, you should see a healthcare provider.Staying Active and Exercising for Back Pain
Staying active is the first thing you can do to ease up your back pain. Regular exercise or movement makes your back flexible and keeps your spine-supporting muscles strong. This also helps in reducing pressure on your joints and bones. Your back may initially experience soreness, but it will not cause any harm. Begin with a mild exercise and gradually increase the duration and intensity. Lack of exercise or movement for a long time makes your muscles weaker and stiffer, leading to a more painful back. Regular exercise gradually eases the back pain. It also releases pain-relieving chemicals - known as endorphins - which not only help in alleviating the pain but also improve the mood. You can also take painkillers with the recommendation of your healthcare provider before performing any exercises. Gradually, you will have a stronger and more flexible back, which will reduce pain.Exercises for Back Pain
There are plenty of exercises you can choose to help relieve your back pain. Some of them are:- Swimming: It is one of the best exercises that is gentle on your back. This low-impact exercise doesn't put too much pressure on your joints, improves circulation and alleviates back pain.
- Walking: It is another way to stay active and relieve your back pain. You can choose the duration and pace according to your comfort and gradually increase them.
- Yoga: It mainly improves your muscles’ stretching and balance, which can be helpful for back pain.
- Pilates: It is also one of the recommended exercises for back pain that improves the flexibility of the body muscles and boosts core strength.
- Gym Workouts: Various workouts that are usually performed at the gym, like strength training and cardiovascular exercises can help improve overall fitness and spine health.
Medications
- Common Pain killers are reducing pain, swelling and inflammation. They are commonly used for the treatment of acute back pain. However, new studies found that these drugs are inadequate in many chronic pain scenarios, while anti-depressants and anti-convulsants can have remarkable effects on many forms of chronic bone and joint pain. Moreover, the addictive potential of opioids must be taken in consideration.
- Muscle relaxants help to release muscle spasm. Thus, the vicious circle of pain – muscle spasm – impaired movement and posture – pain – could be stopped.
- Antidepressants are commonly used and very effective for chronic lower back pain.
- Anti-convulsants (medications to prevent seizures) are successfully used in the treatment of chronic back pain.
Transcutaneous electrical nerve stimulation (TENS)
Transcutaneous electrical nerve stimulation (TENS) is a FDA approved, commonly used method in up-to-date pain management. It’s used for many forms of acute and chronic pain.Acupuncture
Acupuncture may be useful as adjunctive treatment for low back pain.Physical therapy, Massage, Occupational therapy
Physical therapy, Massage, Occupational therapy can be used to alleviate pain and restore function (but this treatment is not encouraged in the early phase of injury)Surgical therapy
Surgical therapy including Lumbar microdiskectomy,Spinal stabilization, Laminectomy, Endoscopic therapy, percutaneous arthroscopic diskectomyCBT (Cognitive Behavioural Therapy)
CBT (Cognitive Behavioural Therapy) was underestimated for a long time but as new studies prove, they are highly effective. In some cases even more effective than medication, with less side effects. A recent study published by the American Psychological Association showed when it comes to chronic pain, psychological interventions often provide more relief than prescription drugs or surgery without the risk of side effects, but are used much less frequently than traditional medical treatmentsLifestyle adjustments
Lifestyle adjustments to eliminate the risk factors, such as obesity, poor physical health, poor nutrition, smoking, heavy manual labor. Support groups are monthly meetings of 5-10 people, having one thing in common, impaired quality of life due to a chronic disease. For psychology and psychiatrist related problems, you can always consult a psychologist, psychiatrist or for counseling our psychotherapists are always available to help you. For psychology and psychiatrist related problems, you can always consult a psychologist, psychiatrist or for counseling our psychotherapists are always available to help you.Sleep Disorders
Disease
Sleep disorder: Insomnia Treatment, Symptoms, Causes & More
Living in Dubai and suffering from insomnia or sleep disorders? We show you how to have a better sleep. But be aware, its actual work!
Every third person in the UAE has at least once suffered from sleep disorders. A healthy sleep is essential for our physical and mental well being. It allows to regenerate the body and to deal with events and emotions endured during the day. But how long does a person need to sleep? Indeed there is no general valid sleep time. Each organism has a biological rhythm thus some are ‘early sleeper’ or ‘late sleeper’. The need of sleep differs according to the person, its age and sleep behavior. However, generally speaking, a person requires 7 to 8 hours of uninterrupted sleep to feel rested.
Definition
Insomnia / sleep disorders are one of the most common complaints in in the world. More than 60 million adults suffer from insomnia just in the U.S. 30% to 50% of the population is affected by insomnia or other sleep problems. Especially in Dubai – a high productive work environment – insomnia is a very common complaint.
Insomnia / sleep disorders are characterized by difficulty falling asleep and/or staying asleep, waking up often during the night, waking up too early in the morning and feeling tired upon waking. It could take a toll on the ability to function during the day and cause an irritability, depression or anxiety. For patients with sleep disorders it is often difficult to pay attention, to focus on tasks or to remember. Insomnia also could cause tension headaches and due to the reduced attention it could increase errors and accidents. Insomnia may be an independent disorder or secondary to a medical condition.
Forms
One distinguishes two forms of insomnia: The primary and the secondary Insomnia. Primary Insomnia is sleeplessness that is not directly associated with any other health condition or problem, like medical, psychiatric, or environmental causes. Secondary insomnia is a result of other causes like illness (Depression, Asthma, Arthritis, Cancer), drugs, excessive worrying, pain. Depression is a leading cause of secondary insomnia.
Moreover one distinguishes between acute and chronic Insomnia. It varies in how long it lasts and how often it occurs. It can come and go and there might be times when a patient has no sleep problems. It varies in how long it lasts and how often it occurs. It can come and go and there might be times when a patient has no sleep problems.
Types
Insomnia: A person suffers from insomnia if he/she has difficulty to falling asleep (sleep-onset insomnia); if the quality and duration of sleep is interrupted during the night or by early waking in the morning and the person is not able to get back to sleep (terminal insomnia).
Disorders of the sleep-wake-cycle: It occurs when the internal hour clock of a person to sleep at dark time and to wake up at light time is confused (e.g. due to time zone change, to shift work)
Parasomnia: It is characterized by abnormal actions or events that occur during sleep (e.g. sleep walking, sleep terrors)
Narcolepsy: It is a neurological disorder expressed by excessive daytime sleepiness.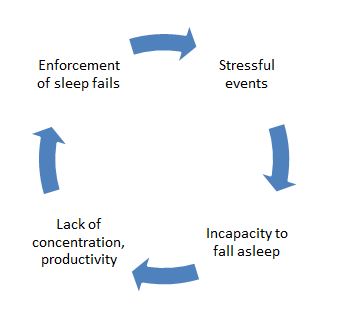
Causes
Causes of secondary Insomnia are mentioned above. Causes of acute primary Insomnia can be emotional or physical complaint, Stress (occupational or private), Illness, Environmental factors like noise, light, or extreme temperatures that impair the quality of sleep, Medications, Interferences in a normal sleep schedule. Causes of chronic primary Insomnia can be Depression or/and Anxiety, Chronic Stress, Pain or discomfort at night.
Often the feeling of tension can cause sleeplessness. Stressful events that have been occurred during the day and not been able to be broken down until the evening can prevent our sleep. A vicious circle starts as the person desires to sleep better on the next day and enforce his/her sleeps but achieves the contrary: a lack of sleep.
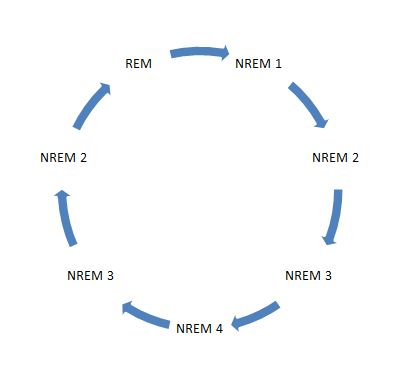 Another reason is the type of sleep. Indeed the profundity and length of a sleep characterizes its quality. Our sleep cycle distinguishes two main phases: The NREM (Non rapid eye movement) phase that has 4 stages going from light sleep to deep sleep and lasts for 90 minutes. This phase helps the body to regenerate. The REM (Rapid eye movement) phase, also known as the dream sleep, that helps to deal with events and emotions endured during the day. A person does not feel rested even if he/she slept 8 hours because the cycle was interrupted: When the person wakes up in the moment of the NREM deep sleep phase, he/she can feel not having got a good night’s rest. Also the regeneration of the body can be affected if the person is not able to reach the deep phase after going to sleep and instead wakes constantly up. The ideal cycle for a reposed sleep is shown in the diagram below:
Another reason is the type of sleep. Indeed the profundity and length of a sleep characterizes its quality. Our sleep cycle distinguishes two main phases: The NREM (Non rapid eye movement) phase that has 4 stages going from light sleep to deep sleep and lasts for 90 minutes. This phase helps the body to regenerate. The REM (Rapid eye movement) phase, also known as the dream sleep, that helps to deal with events and emotions endured during the day. A person does not feel rested even if he/she slept 8 hours because the cycle was interrupted: When the person wakes up in the moment of the NREM deep sleep phase, he/she can feel not having got a good night’s rest. Also the regeneration of the body can be affected if the person is not able to reach the deep phase after going to sleep and instead wakes constantly up. The ideal cycle for a reposed sleep is shown in the diagram below:Finally sleep disorders can also be caused by external disruptive factors: Too low room temperature, too flat/high or too soft/hard pillow, too hard/soft mattress, a ‘low breathable’ duvet are factors of sleep discomfort. Here are some recommendations: It is recommended to air the room before going to sleep. It is important to choose a Pillow that allows the spine to be perfectly aligned. You should use a medium-firm mattress to avoid muscles pressure and offer support to back, neck and legs. If possible, choose duvets made from natural materials (feather, silk, cotton) as they are more breathable and avoid the person to perspire, wake up and have the sleep disturbed.
Diagnostics
Polysomnography is a powerful tool to diagnose sleep disorders. Polysomnography is a comprehensive recording of physiological changes that occur during sleep such as brain waves, oxygen level in the blood, heart rate and breathing rate as well as eye and leg movement. It is used to diagnose or rule out many types of sleep disorders, including Narcolepsy, Restless legs movements, REM behavior, Parasomnias, somnambulism, epilepsy related disease, snoring and sleep apnoea. On the other hand, stress related or other psychiatric disturbances may cause sleep disorders or vice versa, just as inappropriate bedding.
For all these reasons it is of the utmost importance to analyse sleep and sleeping customs thoroughly in order to determine by aid of the neurologist the individually correct diagnosis and ensuing possibilities of treatment for sleep disorders. The sole application of sleeping drugs does not represent an ideal solution but may even be dangerous because it could lead to dependencies as unwanted side-effect.
How to Prepare for the Sleep Disorder Test
There are no major preparations necessary. The patient is advised not to take any sleep medicine or drink alcohol or caffeinated beverages prior to this test.
Risk factors of the Sleep Disorder Test
Polysomnography is a non invasive procedure. There is no risk, except maybe some skin irritation caused by the adhesive used to attach the sensors to the skin. It is therefore a fabulous procedure for children too.
Mechanism of the Sleep Disorder Test
Physiologic sensor leads are placed on the patient in order to record the following:
1. EEG (Electroencephalogram)
2. EOG (Electro-Occulogram)
3. EMG (Electromyogram)
4. ECG (Electrocardiogram)
5. Airflow (thermistor or thermocouple sensor)
6. Respiratory Effort (piezo crystal effort sensor)
7. Oxygen saturation (Pulse oximeter)Procedure of the Sleep Disorder Test
1. AT A SLEEP LABORATORY OR HOSPITAL
For the standard test, the patient - suffering from sleep disorders - comes to a sleep lab in the early evening, and over the next 1–2 hours is introduced to the setting and “wiring up” so that multiple channels of data can be recorded when he/she falls asleep. The sleep lab may be in a hospital, or in a center. A sleep technician should always be in attendance and is responsible for attaching the electrodes to the patient and monitoring the patient during the study. She must explain to the patient about the procedure to keep the patient relaxed throughout the night.
The sleep laboratory should be equipped with video cameras in the patient’s room, so that the patient can be recorded while sleeping. This allows the technician to review the tape at any time during the test and verify whether strange looking waveforms were caused by an actual arousal, a period of wake, or normal patient movements in bed.2. AT HOME
Nowadays, neurologists may carry out home studies to enhance patient comfort and reduce expenses, which is in the best interest of any patient. The patient is given thorough instructions as to how the screening tool is used. He will then use the equipment at home in his usual sleep surroundings and return it the next day. Most screening tools consist of an airflow measuring device (thermistor) and a blood oxygen monitoring device (pulse oximeter). They are small and easy to handle and produce excellent graphs and other results. At the German Neuroscience Center our neurologists follow this new path and provide patients - suffering from sleep disorders - with a tool they can easily apply at home rather than putting the patient into an awkward situation at the clinic because they realize that especially in Arabic countries with prayer times and similar rules to follow, it might be difficult for the patient to carry out a sleep study outside their homes.
The patient will sleep with the screening device for one to three nights, and then return the device to the neurologist. The neurologist will retrieve data from the device and can make assumptions based on the information given, for example, a series of drastic blood oxygen desaturations during night periods may indicate some form of respiratory event (apnea). At a minimum, the equipment will monitor the oxygen saturation.
Sleep Disorder Test SummaryPolysomnography (PSG) has proved to be a convincing tool for enhancing our understanding of sleep and sleep disorders. It is an essential diagnostic procedure to clarify the causes of sleep disorders thus enabling the neurologist to determine an appropriate form of treatment.
Ideally, and in accordance with international guidelines, sleep studies will be carried out by neurologists in close cooperation with an ENT specialist in such cases where first results point at a serious disease, as is standard at the German Neuroscience Center GNC.Evaluation of sleep disorders must be made more readily available to the hundreds of thousands of patients with sleep disorders who still lack diagnosis and treatment. Lack of sleep or permanently disturbed sleep will lead to reduced concentration and failing personal efficiency. This will not only gravely affect the patients’ private lives but also their daily working capacity. Sleep disorders, if not analyzed and left untreated, may lead to dangerous, even fatal, situations and social decline by, for instance, losing one’s job. Today, thanks to Polysomnography, nobody has to take such risks, since our neurologists, psychiatrists, and psychologists at the German Neuroscience Center know of many ways how to treat sleep disorders adequately after having analyzed and diagnosed the causes thoroughly.
Sleep Disorders, Treatment
There are very effective ways of treatment for sleep disorders these days. The problem is rather that patients are hesitant to search professional help. Thus a vicious circle could start where the sufferer is already afraid of going to bed. Obviously then it will be very difficult to fall asleep. If you are suffering from sleep disorders, you know what we are talking about. Specialists are using a combination of these scientifically proven treatment options for insomnia: Sleep hygiene, stimulus control, relaxation techniques, sleep restriction therapy, cognitive behavioural therapy and medications.
We would like to deliver one of these techniques to your doorstep or rather in your bedroom. Stimulus control therapy. It’s very effective and successfully used since more than 30 years. It sounds easy but it’s not. The pivotal point is your willpower to maintain these rules. It is actual work. If you don’t manage it alone, a psychologist might help you.
Rules of stimulus control therapy (Bootzin, 1980)
- Only go to bed when sleepy. Bear in mind being sleepy is not the same thing as being tired. It is important to be aware of this difference.
- Use the bed only for sleep and sexual activity. Do not engage in sleep-incompatible activity in bed such as eating snacks, watching TV or working.
- If after about 10 minutes you are unable to fall asleep or awaken, leave the bed and go to another room. Then return to bed and repeat as often as necessary until you do fall asleep. It is important to not watch the clock while doing this. It is your subjective estimate of time that is important.
- Keep a regular morning rise time no matter how much sleep you got the night before. This will help regularize the circadian (24 hour) schedule and if you don't sleep well one night, the drive to sleep will be higher the following night.
- Avoid napping. This prevents reducing sleep drive earlier in the day that can make it harder to fall asleep at night.
Why is it working? Psychologists call it conditioning. Conditioning is a type of learning that had a major influence on the school of thought in psychology known as behaviourism. Wrong conditioning is a major problem that occurs in chronic insomnia. If you repeatedly toss and turn in your bed for hours on end, your body will eventually learn to associate your bed with stress and being awake. As a result, your bedroom will actually cause you to stay awake. The points above are trying to address this problem and to re-teach your body to associate your bed with healthy sleep. Keep in mind that it takes time and effort to make it work. Like any other form of learning. However, if this is not sufficient a combination therapy might be the right thing for you. This could include sleep hygiene, relaxation techniques, sleep restriction therapy, cognitive behavioural therapy and medication.
Insomnia? Just popping sleeping pills? Bad idea! You should…
Some more tips:
1. Sport and relaxation techniques such as yoga help to get a healthy sleep. It is beneficial to practice them outdoor to get fresh air. However avoid doing sport in the evening or before going to bed, as this would stimulate the body and retard sleep.
2. Do not have heavy meal or stimulating drinks such as coffee, soda or alcohol before going to sleep. Nicotine can also lead to disquietness.
3. Try to relax and unwind before sleep time, switch off from the day, listen to soft music or read light readings. If you cannot stop the flow of stressful thoughts, clean your head by writing your thoughts/do to list/etc. down on a paper, and put the notice in a drawer. This helps to ‘exteriorize’ and ‘lock away’ your thoughts.
4. Before going to bed do not watch animated movies and news or read exciting books.
5. The bedroom should be associated to calmness and tranquility. It is recommended not to have a TV in the bedroom as it is a persistent stimulus.
6. Reduce external disturbing factors such as light or noise.
7. If you are not able to fall asleep eat products rich in magnesium. The best snack would be warm milk with honey and banana.
8. The smell of essential oils (Lavender, Balm or Sandal-wood) appeases the body and enhances sleepiness.
9. If insomnia remains, it is recommended to consult a psychologist who will apply techniques of cognitive behavior therapy. (Cognitive therapy, sleep restrictions, relaxation).
1o. When physical or neurological factors cause sleep disorders, it is imperative to consult a doctor. It is helpful to fill in a ‘sleep diary’ in which you mention bed and wake up time, activities done and food eaten during the day and thoughts or situation that have prevent you to sleep. This diary would provide support to detect the causes of the disorder.
Did You Know?
… that we spend one third of our lifetime sleeping.
…that a person’s body is programmed twice a day to sleepiness: between midnight and 7 am and between 1 and 4 pm.
…that we spend 20-25% of our time dreaming during our sleep.
…that Einstein needed 10-11 hours of sleep and Benjamin Franklin only 4 hours per night!
References:
1. Collop NA, Anderson WM, Boehlecke B, et al. Clinical guidelines for the use of unattended portable monitors in the diagnosis of obstructive sleep apnea in adult patients. Portable Monitoring Task Force of the American Academy of Sleep Medicine. J Clin Sleep Med . 2007;3:737-747.
2. Personal communication: Michael E. Garrison RSPGT, Supervisor Sleep Disorders Center KUMC.
3. Rechtschaffen, Allan. Kales, Anthony. A Manual of Standardized Terminology, Techniques and Scoring System for Sleep Stages of Human Subjects. Brain Information Service/Brain Research Institute. UCLA Los Angeles, CA. 1986.
4. McDonough, James T. Stedman’s Concise Medical Dictionary. 2nd edition. Williams and Wilkins Publishers. Baltimore, MD. 1994.
5.Sheldon SH, Spire J-P, Levy HB. Pediatric Sleep Medicine. W.B. Saunders, Co. Philadelphia, PA. 1992.
6. G. Hayak E. Ruther, Insomnie Schalffosigkeit, 1995.© GNC, German Neuroscience Center Dubai (Neurology, Psychiatry, Psychology, Counseling, Dubai, UAE)
Dementia & Alzheimer’s Disease
Disease
Alzheimer Dementia in Dubai
You fear having Alzheimer’s Dementia? You are suffering from memory loss? You have difficulties to concentrate? Don´t be afraid. To forget things doesn’t mean you are already suffering from Alzheimer Dementia. But what is Alzheimer Dementia actually?
Definition
Alzheimer´s Dementia is a chronic disease of the brain which starts slowly with mild symptoms. One symptom alone is not enough to justify the diagnosis. To forget some things some time does not make an Alzheimer´s Dementia. With ongoing age it is totally normal that your memory becomes worse. When you are 60 years it is more difficult to memorize information than with 50, and with 70 it is more difficult than with 60. That means you forget always a bit more becoming older in a natural way. It is very individual how much and how fast this process is ongoing. This depends on your gens, your general health situation, your environment you live in and your education. In scientific papers is was found that people with high education, university degrees or a sophisticated job, so called “brain workers”, get Alzheimer´s disease more seldom and later than people who work more physically. Our brain has a lot of resources to compensate deficiencies. And a well-trained brain does it better than a “lazy” brain.
Causes
There is not only one disease causing dementia. There are different kinds of dementia diseases like Alzheimer, vascular dementia or Lewy Body Disease Dementia. The syndromes of dementia can also be caused by other diseases like stroke, Parkinson, Hydrocephalus, brain tumor and others. It is the task of a neurologist to find out whether a person is suffering from dementia and if so, which kind. The most common dementia disease is the Alzheimer´s disease. Second most common form of dementia is the vascular dementia or a combination of Alzheimer’s Dementia and Vascular Dementia.
Symptoms
In early stages of Alzheimer´s Dementia patients are not only suffering from decline of memory but also other symptoms. People seem to be depressed because they realize their increasing problems. They feel tired, exhausted and try to avoid intellectual demanding tasks. Already in early stages of Dementia people are changing their behaviour. They are losing interest in things which were important for them before, like their job or hobbies. Patients suffering from dementia are avoiding social contacts, they want to be alone or only with very close persons like family members. The surrounding feels that something is wrong. First it is yet too little to talk or to worry about. There are always excuses to explain the changes. Then when the difficulties become more evident people feel unsecure how to talk about. Alzheimers Disease is stigmatized and for both sides it is difficult to face the facts. For the suffering person the same as for the family members or friends.
Diagnosis
It is important to have a clear diagnosis to either stop worrying or to take action. However, in early stages it can be difficult to differentiate between forgetfulness of age and an early stage of a dementia disease. There are special cognitive tests a neurologist can apply to find out whether the memory alteration is still in age range or not. If there are symptoms of an alteration more than “what is allowed”, further investigations have to be done.
Other diseases like depression, burn out syndrome caused by too much stress, physically exhaustion and other corporal diseases have to be excluded. But how to find out whether a person is suffering from dementia?
First of all go to your neurologist and talk to him about your problems. Already by talking to a patient the doctor gets a first impression. He doesn´t only hear the complaints themselves. Important are also the duration and the progression of the problems. The way how a person speaks, the signs of memory disturbances in conversation, indication of aphasia, disturbance of time or local orientation, all this might already show first straits of a beginning dementia. The doctor also watches the spontaneous behaviour to form his opinion weather it is adapted to the situation or not. It is also important to listen to family members or other close persons. Maybe they have more information the patient eventually already forgot. Or they have another view of the changes the patient did undergo.
Next step are different cognitive tests. For example the worldwide used MMSE (Mini Mental State Examination), a psychometric test to prove orientation, retentiveness, alertness, speech, memory and other function. The neurological examination gives information about the different systems of the brain, peripheral nerves and muscles. Reflexes, speech, gait and locomotor system sensibility, vision, balance and the cranial nerves are checked. It is important to look whether there are any signs which could give an advice for another disease than dementia causing the problems. Blood tests, more seldom examination of the CSF (cerebrospinal fluid) were done. The CSF is the liquid the brain and the spine are covered with all over. In this CSF special peptides can be found which indicate an Alzheimer Disease (Tau-peptide, A beta-peptide).
EEG (electroencephalography) is an examination which does not hurt, comparable to the ECG (electrocardiogram) of the heart. It gives a good overview of the global cerebral function. Other electrophysiological test like AEP (acoustic evoked potentials) or SEP (sensible evoked potentials) can give more information about a lesion in the nervous system to exclude another disease. Also ultrasonic investigations of the cerebral blood flow are part of the diagnostic procedures. The neurologist will send the patient to the imaging of the brain by MRI or CT. In early stages of dementia there are no specific signs for the disease. In more progressed stages you can find signs of atrophy in special parts of the brain (in the temporal area hippocampussklerosis). But the most important reason for the imaging in early stages is again to exclude other diseases which have to be treated in a different way and which might be healed.
Therapy
Therapy of Alzheimer disease is possible. With medication it is achievable to decelerate the progress of the disease, to stabilize the memory, concentration and basic life skills. In Alzheimer Disease nerve cells and nerve cell connections decay which cannot get restored. In consequence of the decay of the nerve cells the messenger substance Acetylcholine decreases. A special kind of medication, the so called “cholinesterase inhibitors”, compensates partly the deficit. By this the information processing improves again. There are other substances which influence the cerebral metabolism in a different way which might also have stabilizing effects on the cognitive functions. Coexisting symptoms like depression, sleeping disorders, anxiety or restlessness have to be treated with other drugs beside the special dementia medication.
Caregivers
Very important is the right contact and handling with the affected person. Lots of patience and sympathy, a quiet surrounding and good information for understanding the disease and the behaviour of the patient are absolutely essential. It is difficult and very exhausting to care for somebody in a more advanced stage when the person needs help in daily activities, in personal hygiene, in nutrition and needs observation the whole day. The family should use all the help and frontline services they could get or attend support groups.
Other than that if you think your problem can be solved by a psychiatrist or a psychologist, you can book an appointment with them as well.© GNC, German Neuroscience Center Dubai (Neurology, Psychiatry, Psychology, Counseling, Dubai, UAE)
.
Stroke
Disease
Stroke, CVA (cerebrovascular accident), CVI (cerebrovascular insult), Brain Attack
Definition
Ischemic stroke, also known as CVA (cerebrovascular accident) or CVI (cerebrovascular insult) or Brain Attack is defined as an interruption of blood flow within one of the brain feeding arteries. Thus the effected brain areas are losing their function and if not treated in time, the nerve cells are dying. Depending on the affected area a stroke can have various clinical signs.
Causes & Risk factors
Most common causes of an ischemic stroke or CVA (cerebrovascular accident) are arteriosclerosis and cardiac embolism following atrial fibrillation. Other causes are vasculitis, arterial dissection or diseases causing hyper-coagulation (blot clotting). There are certain risk factors associated with ischemic stroke or CVA (cerebrovascular accident): age over 60, male gender, Hypertension, Atrial fibrillation, Diabetes mellitus, Dyslipidemia, Cigarette smoking, Migraines.
Symptoms
Symptoms of an ischemic stroke or CVA (cerebrovascular accident) are depending on the affected area of the brain. Often symptoms occur suddenly and are affecting one side. It could be sudden loss of vision, weakness of a limb (paresis), numbness or loss of sensory, problems speaking or swallowing, loss of consciousness, headache, nausea and others. If the symptoms fully recover, the neurologist speaks about an TIA, transient ischemic attack.

Diagnosis
Ischemic stroke or CVA (cerebrovascular accident) is a clinical diagnosis. However, the following tests need to be performed. CT scan or CT angiography, MRI, ECG (Electrocardiography), ECD (Extracranial Duplex Sonography), TCD (Transcranial Duplex Sonography), Echocardiography, blood examinations.
Treatment
The most effective treatment is the prevention of an Ischemic stroke or CVA (cerebrovascular accident). This means reducing the risk factors. To evaluate the risk of Carotid artery stenosis a neurologist can perform a ECD (Extracranial Duplex Sonography), TCD (Transcranial Duplex Sonography). Depending on the findings patients can benefit from interventional therapy, such as carotid endarterectomy. Hypertension, Atrial fibrillation, Diabetes mellitus, Dyslipidemia must be monitored closely and treated correctly. Moreover life stile changes should include: Diet, sports, reducing smoking.
In case a stroke or CVA (cerebrovascular accident) happened, time is the most important factor. Patients must be admitted and treated in a hospital within 3h. First line therapy is i.v. thrombolysis in combination with other medication.
After a stroke or CVA (cerebrovascular accident) happened, patients must take medicine to prevent a second event. This medicine keeps the blood from clotting. Moreover early rehabilitation is determining the recovery. The rehabilitation must be comprehensive and include physiotherapy, speech therapy, occupational therapy and psychology.
Other than that if you think your problem can be solved by a psychiatrist or a psychologist, you can book an appointment with them as well.
© GNC, German Neuroscience Center Dubai (Neurology, Psychiatry, Psychology, Counseling, Dubai, UAE)
Bell’s Palsy
Bell's Palsy Causes, Treatment, Symptoms, Recovery & More
Bell’s palsy is an acute paralysis or weakness of the muscles of one side of the face. It is a relatively common peripheral nerve disorder and can affect people of all ages, but is most common between 15-45 years.
Many celebrities like Angelina Jolie, Anupam Kher, George Clooney, Pierce Brosnan suffered from Bell's Palsy.
Under the right treatment most patients have good recovery, although some are left with residual weaknessSigns & Symptoms
Bell's Palsy causes an acute paralysis of all facial muscles supplied by the seventh cranial nerve (facial nerve). It is always unilateral (one side) and involves upper and lower muscles of the face. At onset people may experiencing mild facial numbness as well. Other symptoms may include:
Read More1) Keratitis (infection of the eye) caused by the failure to close the eye
2) Loss of taste: The tip of the tongue is also innervated by the facial nerve.
3) Sensitivity to loud noises (hyperacusis): The facial nerve innervates the stapedius muscle as well.Causes
Bell's palsy is, by definition, idiopathic, meaning without a specific cause. However, it seems to be associated with certain viral infections. Herpes virus (HSV-1) could be found in 80% of patients. Other viral infections include herpes zoster virus, mumps virus, rubella virus and HIV. Lyme disease has to be taken in consideration as well.
Read MoreRisk Factors
1) Family history (10%)
2) Previous episode (8%)
3) Pregnancy (three-fold risk increase)
4) Diabetes (four-fold risk increase)
Diagnosis
For an experienced neurologist, Bell’s Palsy is mainly a clinical diagnosis. If a virus infection is suspected, blood tests may be considered. If a central paralysis cannot be excluded, a MRI might be considered. To verify the diagnosis and to predict the outcome usually a NCV (nerve conducting velocity) is performed.
Read MoreDifferential diagnosis
Important part of the diagnostic process is to exclude other serious underlying conditions leading to similar symptoms. Differentiating between central and peripheral paralysis is the first step. Stroke and multiple sclerosis as causes for central paralysis have to be exclude.
Treatment
Usually the treatment of Bell's Palsy is very effective and people have a good outcome. However, symptoms can worsen during the first days of treatment. Patients should be aware of this. The outcome of the treatment is better if the treatment is started early. Therapy may include the following:
Read More1) Injections or oral medications are improving the outcome and prognosis
2) Eye protection (a patch and eye drops preventing the eye from getting dry and developing keratitis)
3) Exercises of the affected muscles may improve the progress
4) Surgical decompression is generally not recommendedPrognosis
Usually the outcome of Bell's Palsy is good and most people recover within a few weeks. However, in 8% of the cases the paralysis is recurring.
• Good prognosis: partial paralysis
• Poor prognosis: Complete paralysis, loss of sense of taste after, pathology in the NCV test (nerve conducting velocity)
Complications
Most common complication of Bells Palsy are reinnervation problems. If the nerve is recovering and growing, it may by accident connect to other nerves resulting in malfunctions. This may include:
• Crocodile tears (crying while eating)
• Gustatory sweating (sweating while eating)
• Connection to chewing muscles (face twitching while eating)
Our Team Of Experts
Since more than ten years GNC is the leading clinic for Neurology in the UAE. All our Bell’s palsy experts are German Board Certified and have minimum professional experience of 25 years. If you are searching for the most trusted Bell’s palsy experts, you came to the right place.
We can also help you with the best psychologist, psychiatrist and psychotherapist available in Dubai, UAE.Testimonials
``The doctor is the best and everyone's very helpful``
``Excellent doctor``
``I am thankful for the service.``
``Being able to have blood tests and EEG done at the clinic itself was very helpful and convenient. This also allowed my doctor to have fast access to the test results.``
``I'm impressed by the Professor and team professionalism``
``God bless you guys wish you more of success``
``Great service``
``It was a great visit thanks! It really helped me.``
As Seen On
Epilepsy, Seizures, Convulsions
Epilepsy, Convulsions, Seizures, Fits
Epilepsy, Convulsions, seizures or fits are some of the most common neurological disorders, with an annual incidence of 35 to 52 cases per 100,000 persons. It is a central nervous system disorder that affects the nerve cell activity in the brain characterized by the presence of recurrent, unprovoked seizures.
The patient has a propensity to manifest recurrent episodes of disturbed behavior symptoms and sensations, including loss of consciousness. Seizures or convulsions can have profound physical and psycho-social consequences. However, one single seizure or fit does not indicate Epilepsy.
The disease can only be diagnosed if there is an underlying tendency toward recurrent, unprovoked seizures or fits.
Causes
Epilepsy has no identifiable cause in about half of those with the condition. Specialists speak about symptomatic Epilepsy if they identify a cause like a brain tumor. The most common causes of Epilepsy include:
Read MoreCauses
• Genetic influence
• Congenital abnormalities
• Antenatal or perinatal injury
• Infections such as meningitis, AIDS and viral encephalitis
• Cerebral tumors
• Traumatic brain injury
• Vascular causes (eg, stroke, vascular malformations, cerebral venous thrombosis)
• Inflammatory conditions (eg, vasculitis)
• Alzheimer disease, multiple sclerosis, and other neurodegenerative disorders
Signs & Symptoms
Specialists differentiate between focal or generalized seizures, based on how the abnormal brain activity begins. A focal seizure is characterized by an abnormal activity in just one area of the brain and it could include the loss of consciousness. Generalized seizures are...
Read MoreGeneralized seizures are the most common seizures and involve all areas of the brain and could include symptoms like staring into space or subtle body movements, stiffening of the muscles, a loss of muscle control and an abrupt loss of consciousness, body stiffening and shaking, and sometimes loss of bladder control or biting the tongue.
The general signs and symptoms of a seizure may include:
• Temporary confusion
• A staring spell
• Uncontrollable jerking movements of the arms and legs
• Loss of consciousness or awareness
• Psychic symptoms
Patients may experience an “aura” just before the seizure starts. They may feel “strange”, dizzy or nauseous and can experience changes in mood, visual perception, auditory perception or unspecific symptoms.
Classification
Epilepsy or Seizures are classified as (ILAE):
Read MoreGeneralized seizures
• Tonic–clonic (in any combination) seizures
• Clonic seizures
• Tonic seizures
• Atonic seizures
• Myoclonic seizures
• Myoclonic seizures
• Myoclonic atonic seizures
• Myoclonic tonic seizures
Absence seizures
• Typical
• Atypical
• Absence with special features
• Myoclonic absence
• Eyelid myoclonia
Focal seizures
Unknown seizures
• Epileptic spasms
Diagnosis
Diagnosing Epilepsy is a three-step process involving clinical identification of a possible seizure, consideration of differential diagnoses, and classification of the seizure. The Neurologist will...
Read MoreThe Neurologist will test behavior, motor abilities, mental function and other areas to diagnose the condition and determine the type of epilepsy the patient may have. Moreover, the examination include a blood test, an EEG (Electroencephalogram) and a neuropsychological tests, in which the Neurologist assess thinking, memory and speech skills of the patient to determine which areas of the brain are affected.
Treatment
Most people with Epilepsy can become seizure- or fit-free by taking one anti-seizure medication, called anti-epileptic medication.
The treatment of Epilepsy involves...
Read MoreThe treatment of Epilepsy involves first the establishment of the correct diagnosis and the identification of the syndrome/seizure type. In the second step the Neurologist will determine if medication is necessary and the last step will be to select the right medication. The selection of the right medication is very complex and needs to be individualized on the basis of the type of Epilepsy, patient characteristics and coexisting medical and psychiatric conditions.
However, due to the drug development of recent years there are very efficient possibilities to treat patients with Epilepsy so effectively that the majority can lead an entirely normal life without any seizures or convulsions at all. In severe cases neurosurgical interference may offer help.
© GNC, German Neuroscience Center Dubai (Neurology, Psychiatry, Psychology, Counseling, Dubai, UAE)
Our Team Of Experts
Since more than ten years GNC is the leading clinic for Neurology in the UAE. All our Epilepsy experts are German Board Certified and have minimum professional experience of 25 years. If you are searching for the most trusted Epilepsy experts, you came to the right place.
We can also help you with the best psychologist, psychiatrist and psychotherapist available in Dubai, UAE.Testimonials
``The doctor is the best and everyone's very helpful``
``Excellent doctor``
``I am thankful for the service.``
``Being able to have blood tests and EEG done at the clinic itself was very helpful and convenient. This also allowed my doctor to have fast access to the test results.``
``I'm impressed by the Professor and team professionalism``
``God bless you guys wish you more of success``
``Great service``
``It was a great visit thanks! It really helped me.``
As Seen On
Book Appointment
Tingling, Numbness, Weakness, Pain
You are experience tingling, numbness, weakness or pain and you want to know what’s causing it? This quick guide will explain you how.
Tingling & Weakness in Hands, Feet, Legs Treatment: Symptoms & More
A disease is the underlying cause (i.e. multiple sclerosis), a symptom is how the disease presents itself (i.e. numbness in the limbs)
Tingling, numbness, weakness and pain are the most common symptoms in neurology. Why? Neurology is the science of the nerves (neurons). There are different types of Nerves in the human body:
 Sensory (or afferent) neurons: send information from sensory receptors to the brain. The receptors have different locations and functions:
Sensory (or afferent) neurons: send information from sensory receptors to the brain. The receptors have different locations and functions:1. Eye - Vision
2. Nose – Smell
3. Tongue – Taste
4. Skin, inner organs – Feel, Vibration, Pressure, Pain
Motor (or efferent) neurons: send information from the brain to muscles or glands.
1. Muscles (limbs, heart, blood vessels etc..)
2. Glans (saliva etc..)
The nervous system is controlling all functions of the human body. A nerve damage is resulting in a specific function loss
1. Numbness: damage of a sensory nerve sending sensory information from the skin to the brain
2. Tingling: damage of a sensory nerve sending sensory information from the skin to the brain
3. Pain: damage of a sensory nerve sending sensory information from the skin to the brain
4. Muscle weakness: damage of a motor nerve sending a movement impulse from the brain to the muscles
Ok, tingling, numbness, weakness and pain are the most common symptoms in neurology and they are caused by nerve damages. So far so good. Now it gets a bit more complicated because we want to know where and which exact nerve is damaged. Basically there are 2 different locations possible. The CNS (Central Nervous System – Brain & Spine) and the PNS (Peripheral Nervous System – Nerves of the limbs and inner organs). It’s a bit confusing because:
Both locations can lead to the same symptoms you may experience.
For example blindness. The patient is suffering from vision loss. This can be caused by a damage of the nerve receptors in the eye, the nerve cells leading from the eye to the brain or the nerve cells in the brain itself. Tingling, numbness or pain can be caused by a damage of the nerve receptors in the skin, the nerve cells leading from the skin to the brain or the nerve cells in the brain itself.
Now it gets even more complicated because we want to know the cause of the nerve damage.
The same symptom can be caused by many different diseases.
Numbness can be caused by a squeezed nerve, by neuropathy, by multiple sclerosis or by a brain tumor etc. This shows why it is important to find the exact cause of the nerve damage.
Causes
• Multiple sclerosis
• Stroke, Transient ischemic attack (TIA)
• Migraines
• Seizures
• Nerve Damage (Neuropathy) due to Diabetes
• Nerve injury (i.e. neck injury, back injury)
• Herniated disk in your spine
• Pressure on your nerves (could be due to scar tissue, enlarged blood vessels, infection, tumors or Carpal tunnel syndrome (pressure on a • nerve at the wrist)
• Sitting or standing in the same position for a long time
• Transverse myelitis (inflammation of the spinal cord)
• Encephalitis (inflammation of the brain)
• Abnormal electrolyte levels
• A lack of vitamin B12 or other vitamin
• others
The treatment will be completely different depending on the cause.
Summarizing, we know that tingling, numbness, weakness and pain are the most common symptoms in neurology and they are caused by nerve damages. The damages can be in different locations and they may be caused by different underlying diseases.
How does a neurologist find out what is causing my tingling, numbness, weakness and pain?
In the consultation he will ask you about the symptoms you are experiencing. Onset, pain level, changes during the day or night time, development, location etc… In the neurological examination he will investigate the symptoms and check if they are on both sides, limited to a dermatome, reflexes etc. Moreover for specific damages there are specific neurological examinations like NCV (nerve conducting velocity), Evoked Potentials, MRI etc. Certain diseases like multiple sclerosis require more extensive investigations.
We hope this article could give you a short and not too medical overview of the diagnostic process in case you are experiencing the most common neurological symptoms of tingling, numbness, weakness or pain. In case you have further questions, our team also consists of experienced doctors in psychology, psychiatry and psychotherapy. Please don’t hesitate to contact us.
Nerve Pain & Damage
Squeezed Nerve, Pinched Nerve, Compressed Nerve, Trigeminal Neuralgia
In their anatomical course through the body and the limbs nerves might be damaged in various ways, the cause of damage most often being traumatic. Symptoms of nerve damage may be prickling, numbness and pain but also palsy or disorders of the bladder or the rectum. Lower back pain is one of the most common complaints today. Up to 80% of the US-Population will suffer from back pain at least ones in their lives. Back pain or lumbar pain is the largest cause of work-related absence in the United Kingdom.
Trigeminal neuralgia
Trigeminal neuralgia is a special case of nerve pain. It is often described as the “the world’s worst pain.” Typically, patients suffer from attacks of intense, electric shock-like facial pain along the trigeminal nerve. More information here: Trigeminal neuralgia
Causes & Risk factors
Very often nerves are trapped at the spinal cord, the backbone or in their course to the limbs. The reason for this may be some injury, a slipped disk or the trapping of a nerve in a bony or connective tissue canal. A typical example is the carpal tunnel syndrome.
Symptoms
The symptoms are depending on the location of the injured or damaged nerve. Often nerves in the cervical or lumbar back are squeezed by a slipped disk causing neck or back and leg pain. Another common location is the wrist. If a nerve is squeezed here it results in pain in the hand called Carpal Tunnel Syndrome. But many other conditions can cause nerve damages in different locations such as sports related injuries of the shoulder and others.
Diagnosis
Most important is a consultation with an experienced Neurologist. The clinical impression and physical examination are guiding the way. If the location is identified, certain nerve tests like Nerve Conducting Velocity or Electromyography may be used to verify the diagnosis or to determine the location precisely.

Treatment
All conservative treatment options should be tried before a surgical intervention is considered. These treatment options also depend on the location of the damaged or squeezed nerve. Often specialized physiotherapy, certain braces and life style adjustments are successful. Moreover, an adequate pain management and other medications are essential to optimize a fast recovery. Most nerve damages are successfully treatable without surgery.
Our Team Of Experts
Since more than ten years GNC is the leading clinic for Neurology in the UAE. All our Nerve Damage experts are German Board Certified and have minimum professional experience of 25 years. If you are searching for the most trusted Nerve Damage experts, you came to the right place.
We can also help you with the best psychologist, psychiatrist and psychotherapist available in Dubai, UAE.Testimonials
``The doctor is the best and everyone's very helpful``
``Excellent doctor``
``I am thankful for the service.``
``Being able to have blood tests and EEG done at the clinic itself was very helpful and convenient. This also allowed my doctor to have fast access to the test results.``
``I'm impressed by the Professor and team professionalism``
``God bless you guys wish you more of success``
``Great service``
``It was a great visit thanks! It really helped me.``
As Seen On
Carpal Tunnel Syndrome Treatment in Dubai | GNC
You’ve been plagued by pain, numbness and tingling in your fingers and wrist? You are waking up at night with a “pins and needles” sensation in one hand? There might be other explanations, but the symptoms suggest you may have carpal tunnel syndrome.What is carpal tunnel syndrome?
Carpal Tunnel Syndrome (CTS) is a condition that occurs when pressure is applied on the median nerve and causes sensations of pain, numbness, tingling or weakness in the hand. The median nerve runs along the length of the arm and passes through a narrow passage in the wrist known as the carpal tunnel. If the nerve is compressed in this passage, the nerve might get damaged and symptoms occur. The median nerve is responsible for controlling the movement of your thumb and fingers, except for the little finger. Moreover, it transmits sensory information from the hand and fingers back to the brain.Common Causes of CTS (Carpal Tunnel Syndrome)
There are different causes which can lead to CTS like occupational overstressing of the hands, injuries at the wrist with malposition of the carpal bones, arthritis, pregnancy, diabetes, overweight and others. Also, a genetic predisposition is discussed. In many cases, no single cause can be identified. It may be that a combination of risk factors contributes to the development of the condition. Other causes include:- Hypothyroidism
- Obesity
- Rheumatoid arthritis
- Repetitive movements such as typing
- Diabetes
Carpal Tunnel Syndrome Symptoms
Typical symptoms are numbness or tingling in the thumb, index, middle and ring finger, later pricking and painful paraesthesias. Sometimes the whole arm up to the shoulder is affected. The symptoms are intensified by overloading the hands by repetitive manual work. At the beginning the discomfort can be reduced by “shaking” the hands. Later a persistent numbness may occur. Left untreated, carpal tunnel syndrome can lead to constant pain and to permanent nerve and muscle damage that could severely limit your ability to use your hands. When experiencing CTS in its early stages, you may notice your hands feeling numb as well as a tingling sensation. This happens during the night or after awaking in the morning; but also with certain hand positions like keyboard typing, holding a phone or reading a newspaper, cycling or motor biking. Symptoms could be worsened when holding heavy objects or bending your wrist. Many have reported that shaking their hands may relieve symptoms, but this doesn’t always make the numbness go away completely. When CTS symptoms start to worsen, you might find yourself being unable to have a strong grip when holding objects as the muscles in your hand start to shrink. You may also experience muscle cramping and pain. Other common CTS symptoms include:- Pain, tingling or numbness in your fingers and/or hand
- Weak hands
- Shock-like sensations in your fingers
- Burning or itching sensations in your palm, thumb, or index and middle fingers
- Sometimes the whole arm up to the shoulder is affected
Risk Factors
There are various factors that have been related to carpal tunnel syndrome over the years. These may not directly cause CTS, but do increase the risk of damage to the median nerve. Risk factors include:- Wrist fractures or dislocation
- Arthritis that deforms small bones in the wrist
- Gender; CTS is more common in women as the carpal tunnel area is smaller in women than in men
- Chronic illnesses such as diabetes
- Inflammatory conditions such as rheumatoid arthritis
- Medications
- Obesity
- Pregnancy
- Thyroid disorders or kidney failure
- Workplace conditions that require prolonged and repetitive movement of the wrist, such as typing
Diagnosis
When CTS symptoms develop and start to become unbearable, it is recommended that you visit a doctor. They may conduct tests such as:- Electromyograms, during which doctors will place a thin electrode into your muscle to measure its electrical activity
- Nerve conduction studies to measure the signals in the nerves of your arm and hand
- Ultrasound to look at your tissues and bones
Treatment and Prevention
Treatment for carpal tunnel syndrome will depend on the severity of your symptoms. Doctors may recommend that you:- Make changes to your daily life to avoid repetitive and strenuous wrist movements
- Exercise and stretch more often to help nerves and muscles move better on a daily basis
- Wear a splint if your doctor has advised you to prevent your wrist from moving too much
- Take anti-inflammatory drugs or steroid injections to help reduce swelling and inflammation
- If treatments don’t pan out, you may be recommended to undergo surgery to increase the size of your carpal tunnel and ease pressure on your median nerve.
- Nonsurgical Therapy: Nonsurgical therapy is possible if you have mild to moderate symptoms and the neurological examinations do not show an extensive damage at the median nerve. Medication with anti-inflammatory drugs (NSAIDs) may help relieve pain from carpal tunnel syndrome only in the short term.
- Nocturnal Splint (Wrist Splint): The most effective conservative treatment is nocturnal splinting with a specially wrist splint. If you use it, avoid wearing it all day, since that can weaken your muscles in your wrists and hands. Wearing it all night, however, is recommended. This should be done at least for 3 month.
- Surgery: If the symptoms persist or the nerve conduction velocity becomes worse, surgery has to be considered. Two main types of surgery are used to relieve the pressure on the nerves inside the carpal tunnel: Open Carpal Tunnel Release and the newer Endoscopic Carpal Tunnel Release. Both are outpatient procedures performed under local anesthesia (the surgeon cuts the ligament along the middle of the palm and inner wrist).
Lifestyle Changes and home remedies
These steps may provide temporary symptom relief:- Take short, frequent breaks from repetitive activities involving the use of the hands.
- Lose weight if you are overweight or obese.
- Rotate the wrists and stretch the palms and fingers.
- Take a pain reliever, such as aspirin, ibuprofen (Advil, Motrin IB, others) or naproxen sodium (Aleve).
- Wear a snug, not tight, wrist splint at night. You can find these over the counter at most drug stores or pharmacies.
- Avoid sleeping on your hands.
Alternative medicine
Integrate alternative therapies into your treatment plan to help you cope with carpal tunnel syndrome. You may have to experiment to find a treatment that works for you. Always check with your provider before trying any complementary or alternative treatment.- Yoga: Yoga postures designed for strengthening, stretching and balancing the upper body and joints may help reduce pain and improve grip strength.
- Hand Therapy: Early research suggests that certain physical and occupational hand therapy techniques may reduce symptoms of carpal tunnel syndrome.
- Ultrasound Therapy: High-intensity ultrasound can be used to raise the temperature of a targeted area of body tissue to reduce pain and promote healing. Research shows inconsistent results with this therapy, but a course of ultrasound therapy over several weeks may help reduce symptoms.
Recovery
Most people make a full recovery, but in some cases (fewer than 5 percent) carpal tunnel syndrome recurs after surgery. This happens more commonly following the endoscopic procedure, which often doesn’t open up the tunnel as fully as open release.Summary
If you are experiencing symptoms of carpal tunnel syndrome and you are searching for the most experienced neurologist to diagnose the condition and provide the best treatment, the German neuroscience Center is your clinic of choice. Since more than 15 years GNC is the leading clinic for Neurology in the UAE. All our Carpal Tunnel experts are German Board Certified and have minimum professional experience of 25 years. If you are searching for the most trusted Carpal Tunnel experts, you came to the right place. Book your appointment hereMultiple Sclerosis
Disease
What is Multiple Sclerosis?
Multiple Sclerosis (MS) is an autoimmune disorder in which the immune system of your own body attacks the nerves and especially their myelin sheaths. Myelin damage disrupts communication between nerve cells. Thus functions controlled by nerves could be disabled. As the nervous system is controlling almost all functions of the human body, Multiple Sclerosis may manifest itself through various symptoms. That’s why diagnosing MS is difficult and sometimes takes years. It is an unpredictable, often disabling disease and primarily occurs in young adults between the ages of 20 and 40. MS is twice as common in women as it is in men.
The cause of Multiple Sclerosis is not known but exogenous and endogenous predisposing factors may play a role. Although there is no cure for Multiple Sclerosis treatments can help speed recovery from attacks, modify the course of the disease and manage symptoms.
Multiple Sclerosis and Vitamin D
Vitamin D plays a part in regulating the immune system in the human body. As Multiple Sclerosis is an immune disease, Vit D could have a protective/modulating effect that influences the disease positively. read more
Multiple Sclerosis in UAE | Too Less Sun???
New Australian study showed again the link between too less sunlight / Vit D Deficiency and Multiple Sclerosis. But do we have too less sunlight in the UAE? Since 1974 (Goldberg) researchers are studying the link between too less sunlight and Multiple Sclerosis.
Multiple Sclerosis and Smoking
Studies could show that smoking and passive smoking are risk factor to develop MS. Moreover, patients with MS have a worse prognosis if they smoke compared to non-smoking patients. Furthermore MS drugs are not as effective if patients are smoking. Bottom line: Stop Smoking!
Symptoms
Multiple Sclerosis is often characterized by a relapsing-remitting course, with new symptoms that develop over days or weeks and usually improve partially or completely, followed by a quiet period that can last months or even years.
The signs and symptoms of Multiple Sclerosis vary with one or several of the following:
- Visual blurring, Vision loss, Double vision, pain behind the eye (optic neuritis) The risk to develop MS in the next 15 years is 50%!
- Sensory disturbances, numbness, tingling, pain
- Weakness in limbs, gait problems, incoordination, dysarthria and intention tremor
- Bladder or bowel dysfunction
- Slurred speech
- Dizziness
- Fatigue
Diagnosis
Diagnosing early MS stages can be difficult. MS symptoms can be presented by a variety of other diseases as well. A comprehensive neurological examination should be done in order to rule out other conditions that might produce similar signs and symptoms. The examination includes blood tests, a MRI of the brain and spine and a spinal tap (lumbar puncture) in which a small sample of fluid is removed from the spinal canal for laboratory analysis. This sample can show abnormalities in white blood cells or antibodies that are associated with MS. Moreover, the Neurologist will check motor strength and sensation in all limbs.
Treatment
The treatment of MS is very important even though Multiple Sclerosis is a chronic, potentially debilitating disease with no cure. The treatment focusses on reducing the frequency of relapses and speeding recovery from them. The aim is a slower disease progression and the management of the symptoms. It should be coordinated in consultation with a Neurologist specialized in MS.
There are special medications for the treatment of acute attacks which reduce nerve inflammation. Other medications can lower the relapse rate and reduce the rate of formation of new lesions. Just recently new drugs have been approved for the treatment of MS.
Besides the necessity to apply the appropriate medication in order to alleviate symptoms like palsies, pains, vision disorders, blindness and other neurological symptoms, there are also physiotherapy and other therapeutic measures that can be helpful. However, some patients have such mild symptoms that no treatment is necessary.
Living with Multiple Sclerosis
In order to relief the signs and symptoms of Multiple Sclerosis the patient should try to get plenty of rest and relaxation. Meditation and or deep breathing may help. Moreover, regular exercises can help improve strength, muscle tone, balance and coordination. Swimming, walking, stretching, low-impact aerobics, stationary bicycling, yoga and tai chi are mild to moderate exercise recommended for MS. Exercises also relieve stress which may trigger or worsen signs and symptoms. A balanced diet low in saturated fat but high in omega-3 fatty acids, such as those found in olive and fish oils, may also be beneficial. Studies also suggest that vitamin D may have potential benefits for MS.
If you think that you want to fix something else related to your mental health. GNC Dubai is providing one of the best psychiatrists in Dubai, psychologists in Dubai and psychotherapists in Dubai who can help you find the core reason and in fixing it.MS Support Group Dubai
I've multiple sclerosis but do I look scared?
Young woman with debilitating disease launches forum to help fellow patients. Supported by the German Neuroscience Center the twenty-eight-year-old multiple sclerosis patient Maha Abbas is launching an MS Talks Forum at Dubai's Urban Bistro restaurant this month end to raise awareness about the disease XPRESS, October 14, 2015, Sharmila Dhal, Chief Reporter Dubai: Maha Abbas, 28, is a multiple sclerosis ( MS) patient with a difference.
© GNC, German Neuroscience Center Dubai (Neurology, Psychiatry, Psychology, Counseling, Dubai, UAE)
Parkinson’s Disease
Disease
What is Parkinson’s Disease?
Parkinson’s disease is a progressive neurodegenerative disorder characterized by rigidity, tremor, postural instability, and slowness of movement. It develops gradually, sometimes starting with a barely noticeable tremor in just one hand. Very often the changes in movement are very discreet and therefore an early diagnosis is often difficult. The disease commonly causes stiffness or slowing of movement. Although Parkinson's disease can't be cured, medications may markedly improve the symptoms.

Disease
Symptoms
Parkinson’s disease symptoms may be mild at the beginning and often start on one side of the body. The signs and symptoms may include:
- Tremor (Shaking of the hands)
- Slowed movement
- Muscle stiffness
- Impaired posture and balance
- Loss of automatic movements
- Speech and writing problems
There may be other symptoms such as a reduction of superior intellectual brain functions, psychic symptoms such as Depression but also disorders of vegetative bodily functions.

Disease
Causes
In Parkinson's disease, certain nerve cells (neurons) in the brain gradually break down or die. These certain nerve cells are responsible for the design, the development and the realization of movements. The loss of neurons results in a decreased dopa level in the brain. Dopa is a chemical messenger between nerve cells. The causes of Parkinson’s disease are not known but factors such as genes and environmental triggers may play a role. However, men are more likely to develop the disease than women are and it usually starts around age 60 or older.
Diagnosis
Early diagnosis of Parkinson’s Disease may be difficult as the symptoms are often subtle. The Neurologist will do a comprehensive history and physically examination and order tests to rule out other conditions that may be causing the symptoms. In addition he may give a certain Parkinson's disease medication. Significant improvement with this medication will often confirm the diagnosis of Parkinson's disease.
Treatment
So far, there is no cure for Parkinson’s disease but certain medications can help control the symptoms. They can help manage problems with walking, movement and tremor by increasing the brain's supply of dopa. Depending on the stage of Parkinson’s Disease and the age of the patient different medications are indicated. Certain medications have only a limited effect for a few years. If the effect is not sufficient anymore the medication needs to be augmented or changed.
The main focus of the treatment will be on adequate medication and physiotherapy. Physical exercises are useful therapeutic means. In severe cases neurosurgical intervention might be necessary which is known as deep-brain-stimulation. The surgeons implant electrodes into a specific part of the brain and connect them to a generator implanted in the chest near the collarbone that sends electrical pulses to the brain. Deep-brain-stimulation may reduce Parkinson's disease symptoms.
Living with Parkinson’s disease
It is necessary that the patient works closely with the Neurologist to find the right treatment. Certain lifestyle changes such as a healthy diet and physical exercises may help make living with Parkinson's disease easier. Walking, swimming, dancing, water aerobics or stretching is recommended in order to improve the balance which could be disturbed by the disease. Moreover, some types of alternative medicine such as meditation, yoga, massage, tai chi and acupuncture could be useful tools.
We can also help you with the best psychologist, psychiatrist and psychotherapist available in Dubai, UAE.
© GNC, German Neuroscience Center Dubai (Neurology, Psychiatry, Psychology, Counseling, Dubai, UAE)
Traumatic Brain Injury (TBI)
Traumatic brain injury (TBI) is a consequence of head injury in which a blow to the head results in damage to the brain due to stretch forces. TBI is the leading cause of death in North America for people below 45 years. The UAE has a comparably young population which makes TBI a very common and serious disease.
Many survivors live with significant disabilities, resulting in major socioeconomic burden as well. In 2000, the economic impact of TBI in the US was estimated to be $9.2 billion in lifetime medical costs and $51.2 billion in productivity losses.
Symptoms are often mild and hard to detect. It needs a trained specialist to diagnose and most importantly treat the condition. If treated adequately TBI has very good prognosis.
Causes
• Motor vehicle accidents
• Sport Injuries
• Falls
• Violence
• Military combatSymptoms
Brain injury is a frequently misunderstood injury. Numerous invisible residual complaints are labelled as 'psychological' and are not well understood. A major complaint of brain injury is fatigue and overstimulation.
Overstimulation
We live in a society that is very fast, with lots of stimuli to be processed at a high speed. When someone experiences overstimulation it is harder for them to process stimuli, sounds are perceived as louder and light as brighter. Ambient noise is perceived as irritating, normal sunlight is harder to endure and one gets easily overwhelmed by crowds and lots of movements in their surrounding.
Fatigue
Due to the quick onset of fatigue it can be difficult to go to birthday parties, to go grocery shopping and to participate in social activities. The fatigue causes disturbances in thinking processes and limits the entire functioning. After reading a text, one can already be so tired that one must rest for a period to recover from the mental effort. In particular, the reading of displays (smartphone, computer, tablet) can be highly discomforting to patients who experience brain injury. In addition to the fatigue and overstimulation one notices to have more trouble remembering and concentrating. Memory and concentration becomes harder when fatigue increases.
Secondary Symptoms
When one experiences symptoms but keeps on functioning beyond their own capacity, people can develop secondary complaints. Overstimulation of the brain cannot be compared to overstimulation of the body. The body has, for example, pain signals as a warning signal. The brains gives totally different warning signals like overstimulation by light, noise or crowds, having difficulty processing stimuli, more problems with thinking (concentration and memory) and fatigue. Many people do not recognize these alarm signals, or are not adequately dealing with them and are likely to push through their complaints. The functioning outside their own capacity will further increase the complaints and ultimately exhaustion will occur. Not being able to function in the way as is desired by the patient, the patient can also develop emotional reactions which are often characterized by feelings of powerlessness and frustration. Misunderstood injury thus consists of fatigue, rapidly becoming overstimulated, experiencing a decline in performance and emotional responses.
Misdiagnosing Traumatic Brain Injuries
Brain injury patients are often misdiagnosed or not diagnosed at all. As most professionals are not specialized in diagnosing TBI, the patients hear often “there is nothing wrong”, even if they are suffering from symptoms. Or their symptoms are evaluated as “only psychological”. Not treating TBI adequately will worsen symptoms. This described process is resulting in a major socioeconomic burden (US: $9.2 billion in lifetime medical costs and $51.2 billion in productivity losses).
Diagnosis
Neuropsychological assessment is needed to get a good impression of the 'invisible' residual symptoms and how to cope with them. The neuropsychological examination is used to assess the extent of (mental) energy loss, fatigue, cognitive - / emotional changes and the impact of pain sensations.
At the start of the counseling / therapy an extended interview (anamnesis) with the patient is performed. A broad range of issues are discussed, such as what happened, what are the symptoms, has it been a breaking point in the health perception, which conditions worsen symptoms or affect it. Furthermore, we look at (medical) history, education, type of work, hobbies, social life and how complaints are limiting it. A neuropsychological examination is carried out and on the basis of the results an appropriate treatment plan is suggested. If there is not enough information available, the expertise of many other disciplines can be consulted (neurologists, internists, psychiatrists, etc.).
With this information and understanding, it is possible to establish an adequate treatment involving persons with brain injuries to understand the actual limitations and how to adapt to it.
Treatment
It is important to know that patients themselves often do not have a good understanding of the limitation of their symptoms and complaints, and the patient is driven to perform at pre-morbid level. Recovering from brain damage is a complex process that a patient has to go through with the help of a professional. It is necessary that one acquires knowledge in the presentation of symptoms and also get advice how to deal with it. A brain injury is essentially a neuropsychological phenomenon.
Neuropsychological Rehabilitation
In the next phase, the affected cognitive functions are reactivated and a medical fitness program is used to improve the energy level and reduce pain levels.
Often, the treatment consists of guidance of a clinical neuropsychologist which will provide insight into the complaints and why these occur. Adjustments are taught and exercise / rest schedules are discussed. During the same period, patients will follow medical fitness programs and a cognitrain program. This followed by rest periods. If pain symptoms stay apparent, a neurologist or pain doctor (anaesthesist) is considered. Often the pain sensations consist of pain in the neck and shoulders which also develops into headaches. The progress of each patient is discussed daily and programs are adapted to this feedback. The goal is to become a well- balanced individual again.
To achieve this, the main focus is on personal attention. Our view is that every person is like a fingerprint, completely unique. There is no standard protocol used to provide treatment, as each person has their own way of reacting to all aspects relating to brain injury.
The program usually has a duration of three months and the maximum group size is 12 people. The main goal of a small group is to build a personal relationship with each participant in the program.
If you think that you want to fix something else related to your mental health. GNC Dubai is providing one of the best psychiatrists in Dubai, psychologists in Dubai and psychotherapists in Dubai who can help you find the core reason and in fixing it.
Common Misconception
Often there is a misconception that the complaints of (mild) brain injury will resolve after some time. This natural recovery can only occur when conditions are optimal. One needs to perform the right activities during the recovery period in order to optimize the recovery. It should be noted that even with an optimal recovery period there may be residual complaints!
Neuropathy – Diabetic Polyneuropathy
Neuropathy - Polyneuropathy
Neuropathy is term that describes a damage of the nerves. Most common symptoms include: pain (often worse at night), numbness, tingling, ‘pins and needles’, burning sensation, muscle weakness and others. The damage can be caused by different conditions such as disease, infection, injury, medications, toxins or another reason.
Types of neuropathy
• Peripheral neuropathy affects nerves in outer (peripheral) parts of the body such as the feet, legs, hands and arms.
• Proximal neuropathy affects the muscles of the hips and the shoulders.
• Focal or mononeuropathy affects only one nerve. An example is carpal tunnelsyndrome.
• Polyneuropathy affects several nerves. Most people with neuropathy have polyneuropathy.
• Autonomic neuropathy: Nerves of the autonomic nervous system are damaged leading to symptoms such as problems with digestion, blood pressure and bladder function.
• Diabetic neuropathy is caused by diabetes most commonly affects the nerves of of the hands and the feet. It can also affect nerves controlling automatic functions of the body, such as digestion, or nerves in the hips and thighs.
In the UAE Diabetic Polyneuropathy is the most common type. Therefore, we will describe this type below more extensively.
Diabetic Neuropathy
60-70% of people with diabetes are suffering from Diabetic Neuropathies. Neuropathy may be present even before diagnosing diabetes. Diabetes is the most common cause of peripheral neuropathy in the world. However, the symptoms of neuropathy are mostly unknown to the patients and difficult to diagnose. Early diagnosis is important as diabeticneuropathy can damage any nerve in the human body. Be it the nerves controlling the heart beat or the nerves of the skin. Diabetic skin lesions are the major cause of foot amputation.
Causes
Similar to the variety of symptoms there is also a large variety of causes for this disease. The most frequent reason is a metabolic disorder such as diabetes mellitus. But also hereditary disposition, toxic inhibition or paraneoplastic development can cause polyneuropathy.
Signs & Symptoms
Diabetic Neuropathy means the affection of many nerves due to very different reasons and it can therefore develop many different symptoms. Most frequent are paraesthesia such as prickling, numbness, burning of the feet, but also palsies, disorders of speech and failure of cerebral nerves.
Types of Diabetic Neuropathy
There are different types of neuropathy with different typical patterns of pain distribution. For instance there is the:
Read MoreSymmetric type of diabetic neuropathy
Characterized typically by sensory loss, weakness and painful burning of toes and feet. First symptoms of the symmetric polyneuropathy may appear in the sole of one foot or even involving half a toe, then gradually spreading circumferentially up both legs to the knees, then into thighs and finally the hands. The latter pattern is also termed as “stocking-glove” distribution. Neuropathy always is length-dependent, because the longest axons are the most vulnerable. Patients describe tingling, prickling, burning, numbness and a band like pressure.
Due to sensory deficits, small cuts and wounds will not be noticed by the patients at first thus causing seemingly inexplicable infections. Later, weakness of the muscles will develop, particularly expressed by the fact that patients cannot stand on their heels. With progressing sensory disturbances spreading up also into the tips of the fingers, patients will have difficulties holding objects. Most common is a painful burning in the feet which gets worse with high temperatures. Light stimuli applied to the numb areas may be experienced as extremely painful. Also an imbalance of the gait, getting worse in the dark, is a common symptom of patients with Diabetes.
When the onset of diabetes occurs at a juvenile age of the patients, neuropathies may be first noticed as late as in their thirties to fifties but when the onset takes place at an age over 50, they tend to occur readily with adult-onset. There is a known correlation between the occurrence of neuropathy, the duration and the severity of diabetes, body weight, body size and long-standing hyperglycaemia which must be investigated individually with each patient.
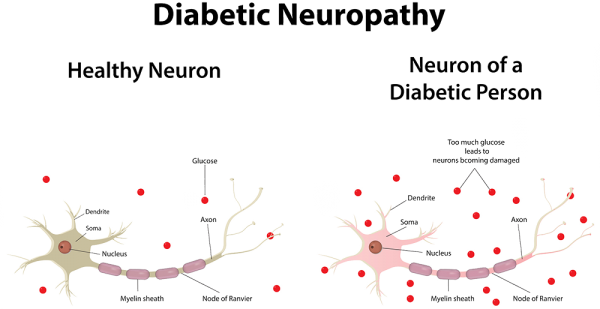
Apart from the above described symmetric form of neuropathy there are other diabetes related neuropathies in different classifications:
Asymmetric diabetic neuropathy
showing focal weakness or sensory loss of single nerves, mainly in one upper arm, one thigh or the cranial nerves.
Asymmetric focal and multifocal types of diabetic neuropathy
of neuropathy are less common, but quite dramatic. They are usually acute in the onset with strong muscle weakness and pain in a thigh or upper arm, but this form rarely occurs before the age of 45. The affection of the cranial nerves causes weakness of the eye muscles accompanied by double images or facial numbness and nerve paralysis.
Autonomic dysfunctions in diabetic neuropathy
Many patients with Diabetes also develop dysfunctions of the autonomic nervous system: constipation, diarrhoea (particularly during the night,), abnormal sweating, hypertension, Tachy- and Bradycardia, dysfunction of the bladder and sexual impotence in males. Symptoms are also uncertain gait, imbalance, maybe syncope’s and blurred vision from lack of papillary regulation.
The distinction between the different kinds of diabetic neuropathy is crucial as far as the different approaches to diagnosis and management are concerned, but also regarding the prognosis.
Treatment
Accordingly, diagnostics and therapy of polyneuropathies are manifold and difficult. The therapeutic aim must be to prevent the deterioration of the nerves itself on the one hand and to treat the illnesses causing polyneuropathy on the other hand. The most essential parts of the evaluation of diagnosis and therapy are...
Read MoreThe most essential part of the evaluation of diagnosis and therapy are – apart from an intensive neurological examination – the electro diagnostic studies of the nerves. The examination comprises Electromyography (EMG) and nerve conduction velocity (NCV). The EMG involves recording electrical potentials by an electrode placed into the muscle, both at rest and during voluntary contractions. The NCV is carried out by stimulating the motor and/or sensory nerves electrically. From the data recorded, informative characteristics of the recorded forms of waves can be determined, thus leading to a clear picture and appropriate treatment.
In the long-term, by way of Diabetes and Complications Control, trial patients who controlled their diabetes meticulously showed significantly less neuropathy. When symptoms of neuropathy occur in patients suffering from diabetes or early signs of polyneuropathic painpatterns as described above, occur, an early neurological examination is of the essence.
Moreover, specialized neuropathic pain treatment can easy the symptoms. Common pain killers are usually not effective enough and anticonvulsants, antidepressants and other drugs need to be used.
Our Team Of Experts
Since more than ten years GNC is the leading clinic for Neurology in the UAE. All our Neuropathy experts are German Board Certified and have minimum professional experience of 25 years. If you are searching for the most trusted Neuropathy experts, you came to the right place.
Testimonials
``The doctor is the best and everyone's very helpful``
``Excellent doctor``
``I am thankful for the service.``
``Being able to have blood tests and EEG done at the clinic itself was very helpful and convenient. This also allowed my doctor to have fast access to the test results.``
``I'm impressed by the Professor and team professionalism``
``God bless you guys wish you more of success``
``Great service``
``It was a great visit thanks! It really helped me.``
As Seen On
Book Appointment
Restless Legs Syndrome
Disease
What is Restless Legs Syndrome?
Restless Legs Syndrome (RLS) is a neurological disorder characterized by an extremely uncomfortable feeling such as creeping, throbbing, pulling, itching or needles and pins in the legs, typically in the evenings while sitting or lying down. It makes the patient feel like getting up and moving around which reliefs the unpleasant feeling temporarily. Restless Legs Syndrome mostly affects the legs, but can also affect the arms, torso, head, and even phantom limbs. It can disrupt sleep and thus leading to daytime drowsiness.
RLS symptoms often begin at the age of 40 years but up to one-third of patients develop symptoms before the age of 20 years. RLS affects estimated 7 to 10 % of the young to middle aged people and 10 to 20 % in those older than 60 years. In the Middle East region approximately 3% of the general population is affected. It is twice as often in women as in men. Especially pregnant women suffer from RLS. 25% of pregnant women develop the disorder in the last three month of pregnancy.
Symptoms
Restless Legs Syndrome symptoms are most commonly located in the deep of the calves, in the feet and thighs. Initially the patient often get an exaggerated sense of positional awareness of the affected leg, later the sensations appear or intensify even while sitting. Movement of the affected part of the body, for instance walking around brings an immediate relief, although temporary and partial and the sensations immediately return after the movement stops. These symptoms often lead to a severe sleep deficiency with secondary tiredness and loss of concentration in job or while driving a car. Some people with severe RLS are not even able to go to work.
Causes
One distinguishes between two kinds of Restless legs Syndrome: the primary and the secondary RLS.
The primary (idiopathic) RLS is a neurological disease with unknown causes. A disturbance of a neurotransmitter system in the brain is suspected. Medication which interferes with the neurotransmitter system helps reliably.
The secondary (symptomatic) RLS is most commonly associated with iron deficiency, venous disorders, polyneuropathy, folacit deficit, Diabetes, renal diseases or pregnancy.
Restless Legs Syndrome can also be induced by antiemetic, anti-depressive and anti-psychotic drugs. A primary RLS should not be considered until possible medical conditions are ruled out, especially venous disorders and polyneuropathy.
Risk Factors
1. AGE. The syndrome affects 10 percent of people 65 and older, compared with only 5 percent of the general population.
2. SEX. Women are more likely to experience the condition than men, but the sex connection seems to be tied to pregnancy. If a woman has never been pregnant, her risk is the same as a man's.
3. LOW IRON. Diminished iron in the brain is implicated in the syndrome.
4. FAMILY HISTORY. People with a family history of the disease are at greater risk.
More than just a discomfort
Harvard researchers found out that sleep deprivation – caused by Restless Legs Syndrome (RLS) – leads to higher risk of early death. Former studies linked RLS with many other conditions, including depression, high blood pressure, and heart disease. This shows that RLS is not just a discomfort or a condition causing sleep problems. It has severe effects on overall health and longevity.
Treatment
The goal of a treatment of Restless Legs Syndrome is to reduce the uncomfortable sensations. Sometimes it is necessary to treat underlying conditions such as iron deficiency or peripheral neuropathy.
With Medication
To reduce the restlessness in the legs there are several medications available such as medications for Parkinson’s disease which reduce the amount of motion in the legs by affecting the level of the neurotransmitter in the brain. Moreover, medications for Epilepsy may help reduce the uncomfortable feeling, as well as muscle relaxants and sleep medications. But these medications don't eliminate the leg sensations, and they may cause daytime drowsiness.
Without Medication
Iron place a big role in Restless Legs Syndrome. Iron levels should be measured and a deficiency should be balanced. Furthermore, a non-medical therapy includes the avoidance of caffeine, alcohol, nicotine, and medications that exacerbate Restless Legs Syndrome, physical activity and good sleep hygiene. Simple lifestyle changes often play an important role in alleviating symptoms of RLS and to learn some relaxation techniques such as yoga and meditation can lead to a significant improvement.
© GNC, German Neuroscience Center Dubai (Neurology, Psychiatry, Psychology, Counseling, Dubai, UAE)
Amyotrophic Lateral Sclerosis (ALS)
Amyotrophic Lateral Sclerosis (ALS), commonly known as Lou Gehrig's disease, is a progressive neurological disorder that affects nerve cells in the brain and spinal cord. At the German Neuroscience Center Dubai, we are committed to providing comprehensive information about ALS to help patients and their families better understand this condition. In this article, we will delve into the signs, risk factors, diagnostics, treatments, and other relevant information to empower patients facing ALS.Symptoms of Amyotrophic Lateral Sclerosis (ALS)
ALS primarily targets motor neurons responsible for muscle movement, leading to a range of symptoms that gradually worsen over time. Common early symptoms include muscle weakness, twitching, and cramping, often in the arms or legs. As ALS progresses, patients may experience difficulty speaking, swallowing, and breathing. Muscle atrophy and loss of motor control are hallmarks of the disease, potentially causing mobility challenges and impacting daily life.Risk Factors of Amyotrophic Lateral Sclerosis (ALS)
While the exact cause of ALS remains unknown, certain risk factors have been identified. Although ALS can affect anyone, it is more commonly diagnosed in individuals between the ages of 40 and 70. Genetics may also play a role, with a small percentage of cases being familial. Environmental factors, such as exposure to toxins or traumatic injuries, have also been linked to a higher risk of developing ALS.Diagnostics
Diagnosing ALS requires a comprehensive evaluation, often involving various medical tests. Neurological examinations, electromyography (EMG) to assess muscle activity, and nerve conduction studies help to identify characteristic patterns of motor neuron dysfunction. Additionally, MRI and other imaging techniques can rule out other potential causes of the symptoms.Treatments of Amyotrophic Lateral Sclerosis (ALS)
While there is no cure for ALS, a multidisciplinary approach can help manage symptoms, enhance quality of life, and provide supportive care. Certain medications may slow the progression of the disease and improve life expectancy. Physical therapy, occupational therapy, and speech therapy can aid in maintaining muscle function and addressing mobility challenges. Assistive devices and adaptive technologies also play a pivotal role in enhancing independence and communication.Supportive Care and Research
ALS patients benefit from ongoing care to address the evolving needs of the disease. Support groups and counseling offer emotional and psychological support for patients and their families, helping them navigate the challenges that ALS presents. The German Neuroscience Center Dubai is actively involved in initiatives to advance our understanding of ALS, leading to improved treatment options and potential breakthroughs.Conclusion
Amyotrophic Lateral Sclerosis is a complex neurological disorder that requires comprehensive management and support. At the German Neuroscience Center Dubai, we are committed to providing patients with the latest information and personalized care to help them navigate the challenges posed by ALS. By understanding the symptoms, risk factors, diagnostics, treatments, and ongoing research efforts, patients and their families can make informed decisions and receive the support they need in their journey with ALS. Contact us today to learn more about our services and how we can assist you in managing ALS effectively.Myasthenia Gravis
Myasthenia Gravis
Myasthenia gravis is an autoimmune disease that causes muscle weakness. The body is producing antibodies which are attacking the junction between nerve and muscle.
Signs & Symptoms
Most common symptoms of Myasthenia gravis are ocular symptoms (50%) of Drooping of the eyelids (ptosis), double vision (diplopia) and blurred vision. The disease can generalize including symptoms like weakness of facial and extremity muscles. Moreover, patients could have difficulties in chewing, swallowing and speech. Respiratory weakness may produce acute respiratory failure.
Read MoreThe symptoms of Myasthenia gravis are negatively influenced by exercise, heat, illness, and stress. Normally they worsen in the evening and get better after resting.

Causes
Often myasthenia gravis is associated with other disease like rheumatoid arthritis, scleroderma and systemic lupus erythematosus. 65% of patients with myasthenia gravis have a hyperplasia of the thymus. 15% of patients with myasthenia gravis present a Thymoma.
Diagnostic procedures
Myasthenia gravis is a clinical diagnosis by specialized neurologist, supported by specific tests including Cholinesterase inhibitor tests, antibody detection test, EMG (Electromyography), Computed tomography (CT) and MRI of the chest, to detect thymoma or thymic hyperplasia.
Treatment
The treatment of Myasthenia gravis is effective and most patients are able to live normal lives. Based on the clinical findings it could include certain drugs (Cholinesterase inhibitors, Immunosuppressant agents, Intravenous immune globulin (IVIG)), Plasmapheresis, Thymectomy, Physical therapy and Lifestyle changes.
Our Team Of Experts
Since more than ten years GNC is the leading clinic for Neurology in the UAE. All our Myasthenia Gravis experts are German Board Certified and have minimum professional experience of 25 years. If you are searching for the most trusted Myasthenia Gravis experts, you came to the right place.
Testimonials
``The doctor is the best and everyone's very helpful``
``Excellent doctor``
``I am thankful for the service.``
``Being able to have blood tests and EEG done at the clinic itself was very helpful and convenient. This also allowed my doctor to have fast access to the test results.``
``I'm impressed by the Professor and team professionalism``
``God bless you guys wish you more of success``
``Great service``
``It was a great visit thanks! It really helped me.``
As Seen On
Double Vision – Diplopia
What is Double Vision?
Patient with double vision see two images of a single object either permanently or intermittent. Double vision is also known as Diplopia. The displacement may be horizontally, vertically or diagonally. The perception of two images can also be overlapping. The symptom of double vision is to take seriously, since some causes need urgent medical treatment.
Symptoms
The symptoms of double vision can vary as described above but depending on the cause, other symptoms may be present with double vision, such as:
• Misalignment of one or both eyes
• Pain with the eye movements in one or both eyes
• Pain around the eyes, such as in the temples or eyebrows
• Headache
• Nausea
• Weakness in the eyes or anywhere else
• Droopy eyelidsCauses
There are many possible reasons for double vision. If the double vision is long-lasting or keeps coming back, reasons for it can include:
• Nerve problems: Multiple Sclerosis, Guillain-Barre syndrome, Diabetes
• Cornea problems: Herpes zoster, Dryness of the cornea
• Lens problems: Cataracts
• Brain problems: Stroke, Aneurysm, Migraine, Brain tumor, Head injury
• Muscle problems: Myasthenia gravisSince the reasons for double vision could be life-threatening, it is very important to consult a Specialist if the symptoms do not stop.
Types
There are three types of double vision: Binocular double vision, monocular double vision and physiological double vision. The eyes of patients with binocular double vision do not work together properly and the double vision will disappear if the patient covers one eye. Monocular double vision occurs when the double vision continues when the unaffected eye is covered. In physiological double vision background objects the patient does not focus on appear doubled. This vision problem often goes unnoticed because the patient's brain can usually compensate for this type of double vision.
Treatment
As many different diseases could lead to the symptom of double vision it can be difficult to find out what the actual cause is. It is important to have a comprehensive examination to determine the cause of double vision. In fact, the condition may be a matter of life or death, such as a brain tumor or aneurysm. Some conditions causing double vision are difficult and sometimes impossible to fix. Some strokes and nerve palsies cause fluctuating double vision that can't be measured accurately enough to correct.
To diagnose double vision and to find out the reason for this symptom the Neurologist will use multiple methods such as blood tests, a comprehensive neurological exam, and possibly imaging studies like CT and MRI. The treatment depends on the findings. If weak eye muscles are the cause for double vision a surgery may help. If Myasthenia gravis or Diabetes is the reason medications will help.
Depression
Disease
Depression
Depression – a disorder as old as the history of humankind. Already Hippocrates (460-377 BC) described melancholia, a condition very similar to today’s depression.
More than 350 million people globally are affected by depression and it can affect anyone – from young people to seniors. But what exactly means being affected by a depression? What are the common symptoms? And which treatments are available?
Definition
Depression is a serious medical illness that causes a persistent feeling of sadness and/or loss of interest. It is also called major depression, major depressive disorder or clinical depression and it affects your feelings, your way of thinking and how you behave. A Depression can lead to a variety of emotional and physical problems, it may make you feel as if life isn't worth living and often it interferes in doing your normal day-to-day activities.
Symptoms
Symptoms can include sadness, emptiness, a loss of interest or pleasure in activities you used to enjoy, a change in weight, a difficulty sleeping or oversleeping, an energy loss, anxiety, agitation or restlessness, slowed thinking, speaking or body movements, feelings of worthlessness and thoughts of death or suicide.
Forms
There are several forms of depression. One distinguishes between a Major Depressive Disorder, Persistent Depressive Disorder (Dysthymia), Psychotic Depression, Postpartum Depression and Seasonal Affective Disorder (SAD).
- Major Depressive Disorder: This form is characterized by a depressed mood which lasts for more than two weeks and which impairs the patient’s life, including work, private life, relationships and friendships. An episode can occur only once in a person’s lifetime, but more often, a person has several episodes.
- Persistent Depressive Disorder (Dysthymia): This form lasts for at least two years and the patient may have episodes of a major depression along with periods of less severe symptoms. This is considered a chronic form of depression.
- Psychotic Depression: This form occurs when a patient has severe depression plus some form of psychosis, such as having disturbing false beliefs or a break with reality (delusions), or hearing or seeing upsetting things that others cannot hear or see (hallucinations).
- Postpartum Depression: This form many women experience after giving birth when hormonal and physical changes and the new responsibility of caring for a newborn can be overwhelming. It is more serious than the “baby blues”.
- Seasonal Affective Disorder: This form is characterized by the symptoms of a Major Depressive Disorder only during a specific time of year, usually winter. This appears to be related to the shorter days of winter, and the lack of sunlight in many parts of the country.
A depression is more than just a “blues” or feeling down for a few days. It is a medical illness, not a sign of weakness.
Causes
There are a number of factors that may increase the chance of depression but it is not known exactly was causes this illness. Factors that could be involved are biological differences, brain chemistry, hormones, inherited traits and life events. Most likely, depression is caused by a combination of these factors. It is supposed by longstanding theories about depression that important neurotransmitters - chemicals that brain cells use to communicate - are out of balance. Brain-imaging technologies, such as magnetic resonance imaging (MRI), have shown that the brains of people who have depression look different than those of people without depression. The parts of the brain involved in mood, thinking, sleep, appetite, and behavior appear different.
Moreover, the risk for depression could result from the influence of several genes acting together with environmental or other factors as research indicates. In addition, trauma, loss of a loved one, a difficult relationship, or any stressful situation may trigger a depressive episode. Other depressive episodes may occur with or without an obvious trigger.
Treatment
A comprehensive physical examination by a doctor should be the first step of getting a treatment to rule out other possible causes for the symptoms. Next a diagnostic evaluation for depression should be conducted by a Psychiatrist or a mental health professional. The treatment depends on the type of depression that you may be suffering from. For example, some patients with a clinical depression are treated with psychotherapy and others are prescribed antidepressants. Still others who don't respond to standard depression treatments are treated by brain stimulation techniques such as electroconvulsive therapy (ECT), also called electroshock therapy, transcranial magnetic stimulation (TMS), or vagus nerve stimulation (VNS).
However, you should be aware that depression will not be cured in only one day or with only one pill. Being patient is important and trying different antidepressant may be required to find the most effective one for you. Psychotherapy is an effective treatment but on its own it may not be enough to resolve severe depression. But it can play an important role when used with other treatments, including medications.
If you're unable to know what your mental health concer is, we can help you with that using our top Neurologists & psychologists help.© GNC, German Neuroscience Center Dubai (Neurology, Psychiatry, Psychology, Counseling, Dubai, UAE)
Child & Adolescent Mental Health
Trigeminal Neuralgia
Trigeminal neuralgia is a special case of nerve pain. It is often described as the “the world’s worst pain.” Typically, patients suffer from attacks of intense, electric shock-like facial pain along the trigeminal nerve.
Causes & Risk factors
Although the exact cause of trigeminal neuralgia is not fully understood, research indicates that the trigeminal nerve is damaged by a loss of myelin, in some cases caused by a blood vessel compressing the nerve. Other causes include multiple sclerosis, stroke, brain trauma and others.
Symptoms
Trigeminal neuralgia patients suffer from attacks of intense, electric shock-like facial pain along the trigeminal nerve. These attacks can occur without warning signs and last from seconds to minutes. In some cases, they might be trigger by touching the face, talking, eating, drinking, shaving or brushing teeth and other activities.
Diagnosis
In case of trigeminal neuralgia, most important is a consultation with an experienced Neurologist. The clinical impression and physical examination are guiding the way. If the location is identified, certain nerve tests like Nerve Conducting Velocity or Electromyography may be used to verify the diagnosis or to determine the location precisely.
Treatment
First line treatment for Trigeminal neuralgia are certain medications such as anticonvulsants, antidepressants, injections etc. Usually, those have a good response rate over 85%. Only in cases of remaining pain surgery should be considered. There are various types of surgery available nowadays. Most surgeries are leading to a complete destruction of the nerve, which causes facial numbness. Therefore, surgery should be only considered if all other treatment options failed.
Our Team Of Experts
Since more than ten years GNC is the leading clinic for Neurology in the UAE. All our Trigeminal Neuralgia experts are German Board Certified and have minimum professional experience of 25 years. If you are searching for the most trusted Trigeminal Neuralgia experts, you came to the right place.
We can also help you with the best psychologist, psychiatrist and psychotherapist available in Dubai, UAE.Testimonials
``The doctor is the best and everyone's very helpful``
``Excellent doctor``
``I am thankful for the service.``
``Being able to have blood tests and EEG done at the clinic itself was very helpful and convenient. This also allowed my doctor to have fast access to the test results.``
``I'm impressed by the Professor and team professionalism``
``God bless you guys wish you more of success``
``Great service``
``It was a great visit thanks! It really helped me.``
As Seen On
Memory Loss, Memory Problems & Forgetfulness
Memory loss and memory problems such as Forgetfulness can be concerning, affecting various aspects of daily life. Prompt medical evaluation is crucial when encountering memory problems. As a premier neurological center in Dubai, the German Neuroscience Center is committed to providing comprehensive information about memory issues. In this article, we delve into the signs and symptoms, risk factors, causes, diagnostics, treatments, and other relevant information for patients experiencing memory challenges.Memory Loss: Signs and Symptoms
Memory issues can manifest in several ways, with varying degrees of severity. Common signs and symptoms include:- Forgetfulness: Frequent forgetfulness of recent events, appointments, or conversations.
- Difficulty Concentrating: Struggling to focus on tasks, making decisions, or following conversations.
- Confusion: Feeling disoriented or confused about time, place, or people.
- Misplacing Items: Frequently losing or misplacing items in unusual locations.
- Repetitive Questions: Asking the same questions repeatedly within a short span of time.
Risk Factors for Memory Problems
Certain factors increase the likelihood of experiencing memory problems, including:- Age: Advanced age is a common risk factor for cognitive decline and memory issues.
- Medical Conditions: Conditions like Alzheimer's disease, vascular dementia, and mild cognitive impairment can contribute to memory problems.
- Family History: A family history of cognitive decline or neurodegenerative disorders can increase the risk.
Common Causes of Memory Issues
Memory problems can stem from various underlying causes:- Neurological Conditions: Neurodegenerative disorders like Alzheimer's and Parkinson's disease can affect memory.
- Depression and Anxiety: Mood disorders can impact memory and cognitive function.
- Medications: Certain medications have cognitive side effects that affect memory.
- Sleep Disorders: Inadequate sleep or sleep disorders can impair cognitive function.
Diagnostics and Evaluation
Diagnosing memory problems requires a comprehensive evaluation, including:- Medical History: Gathering information about medical conditions, medications, and family history.
- Cognitive Tests: Assessing memory, attention, and problem-solving skills through specialized tests. At the German Neuroscience Center we offer the most advance neuropsychological testing to detect early memory loss and mild cognitive impairment.
- Imaging: Brain imaging techniques like MRI and PET scans can reveal structural abnormalities.
- EEG (Electroencephalography): EEG measures the electrical activity of the brain by recording the signals produced by neurons using electrodes placed on the scalp. This activity is displayed as wave patterns, which provide insights into brain function and potential abnormalities. EEG is a non-invasive procedure that is safe and painless, making it a valuable tool for diagnosing and monitoring dementia. Different types of dementia, such as Alzheimer's disease, vascular dementia, and Lewy body dementia, often exhibit specific EEG patterns. EEG can aid in distinguishing between these different forms of dementia based on the unique electrical signatures associated with each type.
- Laboratory Tests: Blood tests can identify underlying medical conditions contributing to memory issues.
Treatment Approaches for Forgetfulness & Memory Loss
The approach to treating memory problems depends on the underlying cause and severity:- Lifestyle Modifications: Adopting a brain-healthy lifestyle with regular exercise, a balanced diet, and adequate sleep.
- Cognitive Rehabilitation: Engaging in cognitive exercises to improve memory and cognitive function.
- Medications: In some cases, medications can help manage symptoms or slow the progression of underlying conditions. Lately some promising drugs received the FDA approval and can be used depending on the individual case.
- Therapies: Behavioral therapies, counseling, and support groups can aid in coping with memory challenges.
When to See a Doctor
Prompt medical evaluation is crucial when encountering memory problems:- Persistent Symptoms: If memory problems persist or worsen over time, consult a doctor.
- Disruption in Daily Life: If memory challenges hinder daily tasks, work, or relationships, seek medical attention.
- Sudden Changes: Rapid onset of memory issues or cognitive decline requires immediate medical assessment.
- Concerns about Loved Ones: If you notice memory problems in a family member or friend, encourage them to seek help.
Conclusion
Memory loss and memory problems can impact individuals of all ages, affecting daily functioning and quality of life. At the German Neuroscience Center Dubai, we offer specialized care and support for those experiencing memory challenges. By recognizing the signs, understanding risk factors, and seeking timely evaluation and treatment, individuals can proactively address memory issues and enhance their cognitive well-being. Our dedicated team of neurologists is committed to providing personalized care to help patients navigate the journey toward improved memory health. Contact us to book your appointment now.Anxiety, Phobia, Panic Attacks
Disease
Anxiety, Phobia, Panic Attacks, Agoraphobia, Fear
Anxiety, Phobia, Panic Attacks and Agoraphobia have one thing in common. Fear. Fear is a feeling that everybody knows as being an entirely normal feeling. Fear usually is a reaction to a frightening situation such as a bank robbery or any other dangerous situation. Normal fear turns into anxiety disorders or phobia when a fearful reaction occurs that does not correspond to the actual event, i.e. a situation that the majority of people would rate as not frightening at all, or if the anxiety reaction is so abnormally strong that the patient has the impression he is going to vomit, to faint, to die or to go insane.
Definition and Symptoms & Signs
Panic attacks
Panic attacks are unexpected short attacks of fear. The duration can be between 10 -20 minutes. The patient often experiences palpitations, chills or hot flushes, sweating, trembling or shaking, nausea, dizziness, numbness or tingling. Moreover the patients could experience shortness of breath and chest pain. This could lead to fear of having a heart attack, fear of choking, fear of losing control, fear of losing one’s mind, fear of fainting and fear of dying. Patients are not able to say what they fear in particular. Thus they are worried that it could happen again. Panic attacks can occur as panic disorder or be a symptom of other conditions like phobias or post-traumatic stress disorder.
Agoraphobia
Agoraphobia describes the fear of being trapped and not being able to escape certain situations or places while having a panic attack. These situations could be: being far from home or travelling, being in crowded places, standing in a line, being on a bridge. Thus patients are trying to avoid all these situations up to the point where they are restricted in almost all activities of daily living or even being housebound. Symptoms are sometimes less troublesome if patient is accompanied by a trusted friend or a family member
Panic disorder
We speak about panic disorder if panic attacks are recurring or if the patient is constantly worrying that another panic attack will follow. We separate panic disorder with agoraphobia from panic disorder without agoraphobia.
Associated disorders
Depression
Often patients with severe or long-lasting panic attacks / disorders develop a depression. The risk is 10 times higher than in the average population. This leads to an increased suicide attempt rate of 20%
Alcohol and substance misuse
Often patients with severe or long-lasting panic attacks / disorders develop dependencies or misuse of alcohol or other substances. The risk is 2 times higher than in the average population.
Diagnostic
It is important to exclude or rule out all organic / physical causes of the symptoms presented like a heart attack etc. Therefore it could be necessary to perform: physical examination, blood pressure, comprehensive laboratory tests, ECG, Echocardiogram, EEG, CT, MRI.
If you're unable to know what your mental health concern is, we can help you with that using our top Neurologists, psychologists & Psychiatrists help.Treatment
There are very effective ways of treatment for panic attacks / fear related disorders. Best practice is the combination of the following:
Psychotherapy
Cognitive behavioral therapy (CBT) & exposure therapy is the first-choice treatment and showed improvement in70-80% of the patients.
Medication
Antidepressants are the first-choice medication. Up to 85% of patients showed improvements. Other medications are very powerful on short term basis and are showing significant reduction of the symptoms and fear.
Lifestyle changes
Stress management programs and Support groups are a big help for patients suffering from panic disorders.
© GNC, German Neuroscience Center Dubai (Neurology, Psychiatry, Psychology, Counseling, Dubai, UAE)
ADHD – Attention Deficit Hyperactivity Disorder
Disease
ADHD - Attention Deficit Hyperactivity Disorder
Approximately 5 to 10% of children between the ages of 6 and 18 years are affected by ADHD. Boys are 3 to 4 times more affected than girls. For a long time people believed that ADHD occurs solely during childhood. But in 30% of the affected children the symptoms persist – possibly in a milder form -, frequently combined with additional psychiatric disorders as depressions, anxiety disorders or dependencies. Adults with ADHD are often not diagnosed until a diagnosis has been made for one of their children.
Attention-Deficit/Hyperactivity disorder is a neurobiological brain function disorder, which often causes significant implications for the affected person’s professional and private life. It is presumed that this condition is caused by an imbalance between individual neurotransmitters leading to disturbed information processing between different areas of the brain, which are responsible for concentration, conception, and impulse control. Hence new information can be less well filtered and the persons affected become constantly over-stimulated. They are struggling to distinguish what is important from what is unimportant and is hard for them to focus on main points. Due to the high rate of occurrence within families a genetic predisposition does probably exist, but birth asphyxia and other environmental influences are said to be contributing elements, too.
ADHD Symptoms:
Attention deficiencies and disorganisation: Lack of concentration while reading longer texts – work instructions! -, difficulty following longer conversations and lectures attentively. A person with ADHD becomes even more distracted while performing subjectively boring activities, for example routine activities. New tasks are continually being started with older tasks not being finished, preventing the formation of patterns, which would be required for establishing structures. This implies disorder and chaotic organisation: The persons affected are not able to multitask, they have problems to organise their daily life and they have poor time management skills. They frequently change jobs, interrupt their life career and generally even face financial difficulties. In their private lives they are often unhappy in relationships, break up with their partners more often, have unstable friendships and have difficulties parenting their own children, too. The consequences are reduced self-esteem and feelings of failure.
Hyperactivity: is generally less pronounced in adults, but can reflect in the inability to remain seated for longer periods (flights, cinema, lectures etc.). The affected persons often jiggle feet or tap the table with their fingers.
Impulsiveness and labile affect: Emotional liability and hyperexcitability with rapidly changing moods up to several times per day may occur spontaneously but can also be initialised from the outside. The affected persons react extremely emotionally to daily stress factors; they are impatient with others, interrupt their counterpart during a conversation, are increasingly irritable, have a low frustration tolerance and tend to risky driving behaviour. On the other hand: Adults with ADHD are often very creative and have associative thinking abilities. When they are occupied with tasks they are interested in, they can work extremely hard and persistently. They even become specialists on many occasions. They are very sensitive towards interpersonal vibrations, can be very empathetic, enthusiastic and impulsive.
ADHD Treatment
There are various therapeutic options, as for example concentration techniques, self-organisation techniques and conflict management training. The treatment should be customized for each individual according to their specific needs. Moreover, education of patients, families, and teachers regarding the diagnosis is an integral part of treatment. In more severe cases medication might be required.
The treatment is focused on improvements in daily life, education, job, career, personal and family life.
© GNC, German Neuroscience Center Dubai (Neurology, Psychiatry, Psychology, Counseling, Dubai, UAE)
Eating Disorders
Disease
Eating Disorders, Bulimia nervosa, Anorexia nervosa
What are Eating Disorders?
Eating Disorders are conditions defined by abnormal eating habits that may involve either insufficient or excessive food intake to the detriment of an individual’s physical and mental health. Bulimia nervosa, anorexia nervosa and binge-eating disorder are the most common specific forms of eating disorders.
Eating disorders can cause serious physical problems and they can even be life-threatening. Most commonly they appear during the teen years or young adulthood but may also develop during childhood or later in life.
Types and Symptoms
Anorexia nervosa
Anorexia nervosa is characterized by abnormal eating behavior, an obsession with food and being thin, sometimes to the point of deadly self-starvation. A person with Anorexia has an intense fear of gaining weight, a distorted body image, a self-esteem that is heavily influenced by perceptions of body weight and shape, or a denial of the seriousness of low body weight. Even if a patient is underweight he sees himself as overweight. Moreover, the disease is characterized by a refusal to eat and denial of hunger, excessive exercise and a fear of eating in public.
Physical consequences of Anorexia nervosa could include the thinning of the bones (osteopenia or osteoporosis), brittle hair and nails, dry and yellowish skin, growth of fine hair all over the body (lanugo), low blood pressure, slowed breathing and pulse, damage to the structure and function of the heart, brain damage, multiorgan failure and infertility.
Bulimia nervosa
Bulimia nervosa is characterized by episodes of eating large amounts of food in a short duration followed by forced vomiting, excessive use of laxatives or diuretics, fasting, excessive exercise, or a combination of these behaviors. People with this disease may be at a normal weight or even a bit overweight, although they often fear gaining weight, desperately want to lose weight and intensely are unhappy with their body size and shape.
Physical consequences of Bulimia nervosa could include a chronically inflamed and sore throat, swollen salivary glands in the neck and jaw area, abnormal bowel functioning, damaged teeth and gums, irregular heartbeat, menstrual irregularities or loss of menstruation and an electrolyte imbalance which can lead to heart attack.
Binge-eating disorder
People with Binge-eating disorder lose control over eating. They eat excessive amounts of food (binge), but unlike Anorexia and Bulimia they don't try to compensate for this behavior with exercise, fasting or purging. Binge-eating disorder is characterized by eating to the point of discomfort or pain, eating faster and frequently eating alone.
As a result, people with binge-eating disorder often are over-weight or obese. They are at a higher risk for developing cardiovascular disease and high blood pressure. Moreover, people with this disease often feel depressed, disgusted or upset over the amount eaten. They experience guilt, shame, and distress about their binge-eating, which can lead to more binge-eating.
Causes
The causes for eating disorders are manifold. Possible causes include biological reasons, psychological and mental health and society. There may be genes that make certain people more vulnerable to developing eating disorders. People with these disorders may have psychological and emotional problems such as a low self-esteem that contribute to the disorder. Moreover, society often cultivates a desire for thinness, especially in the modern Western culture.
Treatment
Psychotherapy, nutrition education and medication are effective treatment methods for eating disorders. An individual, group or family psychotherapy helps the patient to learn how to exchange unhealthy habits for healthy ones. The main focus of the treatment is to restore the person to healthy weight, treating the psychological issues related to the eating disorder and to reduce or eliminate behaviors or thoughts that lead to insufficient eating and preventing relapse. Cognitive behavioral therapy is commonly used in eating disorder treatment, especially for bulimia nervosa and binge-eating disorder.
Eating disorders can’t be cured by medications but they may help to control urges to binge or purge or to manage excessive preoccupations with food and diet. Since eating disorders often occur along with depression and anxiety medications such as antidepressants, anti-anxiety and mood stabilizers may also help with these symptoms.
© GNC, German Neuroscience Center Dubai (Neurology, Psychiatry, Psychology, Counseling, Dubai, UAE)
Bipolar Disorder
Bipolar Disorder
Bipolar disorder, formerly known as manic-depressive disorder, is a quiet commonly used term these days. Many famous people declared to suffer from it; such as Robin Williams, Mel Gibson, Catherine Zeta-Jones, Amy Winehouse, Sinéad O'Connor, Britney Spears, Jean-Claude Van Damme, Axl Rose, Russell Brand, Richard Dreyfuss and many more. Moreover, many historical personalities are believed to have suffered from bipolar disorder; such as Frank Sinatra, Ernest Hemingway, Vincent van Gogh, Friedrich Nietzsche, Florence Nightingale, Edvard Munch, Edgar Allan Poe and many more.
Bipolar disorder seems to be a common disease that everybody knows somehow. But what are the facts? In this article we would like to give you an overview over the disease and answer the most common question.
Definition
As the name suggests, Bipolar Disorder is a mood disorder where patients can show both poles of the mood span alternating. Meaning patients could switch frequently from mania (“too happy”) to depression (“too sad”). But what is “too” happy or “too” sad? Who decides if it is a normal mood or a disease? The answer is clear. The suffering itself defines the disease. Meaning, the right question to ask should be: Is anybody suffering? The patient itself or the surrounding? If nobody is suffering it is absolute fine to be sad or happy sometimes. It belongs to life. The situation changes if somebody is suffering from its sadness or even is at the point to commit suicide because the suffering is so extreme that it appears like there is no way out. These people have the right and they should have an easy access to professional help. There should be no stigma holding them back. It’s not a weakness or failure in any kind. The same is applicable for the surrounding. If other people suffer from the behaviour of somebody else, they should have the possibility to express their suffering and search help; e.g. your spouse is so “happy” that he gambles away your whole savings because he continuously believes to be “lucky” the next time. Or a pilot who is so “happy” and over-confident that he believes that he doesn’t need sleep or any kind of safety measures anymore before flying you to your holiday destination. In these situations the patient himself won't suffer but there is a possibility that others will.
It is not a psychiatrist or any other doctor who decides in first place if somebody is mentally ill. It’s the patients themselfs and their surrounding.
Facts
Even though many successful people are suffering from bipolar disorders, it is a serious disease. Some facts: 11% to 15% of untreated patients are committing suicide. Up to 50% attempt suicide. More than 50% will develop drug or alcohol misuse. The divorce rate is increased three-fold. 50% will be unemployed 6 months after a manic episode. 800 out of 100,000 People living in the U.S. are suffering from it. Onset is most commonly between 15-24 years. Both sexes are equally affected. Bipolar disorders are more common in urban areas and in upper socioeconomic classes and higher educated people.
Causes
The causes of bipolar disorders are still unknown. Most probably there won’t be a single cause but a multifactorial genesis. The Stress-Vulnerability-Coping Model is a commonly used model to explain mental illnesses. Scientists could identify many different risk factors; like a positive family history of bipolar disorder. Patients whose father or mother suffered from bipolar disorder have a 20% higher risk to develop it as well. Moreover childbirth was discovered as a risk factor. 45% of women suffering from bipolar disorder had their first episode in the postpartum period. Stress - be it physical (eg physical illnesses) or psychological (eg work, relationship etc.) - seems to be a risk factor; as well as drug or alcohol abuse.
Symptoms and signs
Depression: The ICD-10 defines 3 major symptoms which are depressed mood, Loss of pleasure and interest in activities and Fatigue or loss of energy. Other symptoms could be lack of concentration and memory, hopelessness, feelings of guilt and unworthiness, suicidal tendencies, sleep disorders, loss of appetite and weight.
Mania: The ICD-10 defines 2 major symptoms which are abnormally euphoric mood or irritated mood. Further symptoms could be lack of concentration and distractibility, racing thoughts, poor judgment, reckless behavior, increased impulsivity, inflated self-esteem, increased energy, increased activity, hyperactivity, rapid speech, reduced need for sleep, increased libido and hyper sexuality.
Psychotic symptoms: in both episodes it is possible that psychotic symptoms occur.
Forms
Bipolar I disorder is described as the combination of 2 or more episodes of Mania and Depression or mixed episodes.
Bipolar II disorder is described as the combination of 2 or more episodes of Hypomania and Depression or mixed episodes.
Rapid cycling bipolar disorder is described as the combination of 4 or more episodes of Mania and Depression or mixed episodes in one year.
Ultra rapid cycling bipolar disorder is described as the combination of 4 or more episodes of Mania and Depression or mixed episodes in one month.
Diagnosis
As in any mental illness first severe organic causes have to be ruled out. This should be done by a Psychiatrist in Dubai and include physical examination, blood tests and the MRI of the brain should not be older than 1 year. If medication should be used other diagnostic procedures may be applicable like EEG or ECG. In the second step the psychiatrist will do psychiatric examination and evaluate based on the ICD-10 or the DSM-IV the symptoms. Moreover there are neuropsychological tests available to evaluate the symptoms of manic or depressive episodes under the supervision of our top Neurologists in Dubai.
Treatment

There are very effective treatment options for bipolar disorders. The priority is to protect the patient and his surrounding from any kind of risk. Be it the sufferer itself from risky behaviour or suicide; be it his surrounding from reckless behaviour or abuse. Without adequate treatment the average woman suffering from bipolar disorder will lose 9 years of life, 14 years of effective activity, and 12 years of normal health. This is due to the fact that bipolar disorder is a chronic disease. Over 90% of people who have an episode of mania will have another. The earlier the onset, the worse is the prognosis. With treatment 90% will improve, 50% will be symptom-free.
But before going into detail, let’s have a look at the biggest obstacles on the way to get there.
Therapy motivation. The most complicated step is always the first one. Searching professional help is a difficult step for most people. It seems that the stigma of mental illnesses is widely present. Moreover the inside that treatment could be necessary is particularly in manic episodes often not sufficient. Even if the surrounding is suffering from the behaviour of the patient, the patient in a manic episode could not be aware of it. It is a difficult task for caregivers to convince the patient that there might be something wrong. Often the patients realize the consequences of their behaviour only after the manic episode is over or if it has severe consequences like jail terms or health damages. While suffering from a depressive episode the drive is often reduced to the extent that patients are not able to search for help by them self’s. This shows the importance’s of the caregivers in bipolar disorders.
The next obstacle is the maintenance of a successful therapy. Even if the patient discovered that treatment helped, it is common that they will stop medication at some point. One-third to one-half of bipolar patients stop medication against advice. As bipolar disorder is highly recurring, there is a high risk of relapse.
Pharmacotherapy
In Bipolar disorder different types of medication are used. The treatment is always individual and depends on many factors, such as experienced effects in the past, side effects, current episode, severity of symptoms etc. Commonly used medications are Mood Stabilizer, Antidepressants, Anticonvulsants and Benzodiazepines. An average treatment period could be 12 month in patients with a low risk of relapse and 5 years to indefinite in patients with high risk of relapse.
Psychology
Medication should always be combined with some kind of psychological support. It is important to establish a reliable relationship to your healthcare professional and to develop a realistic treatment plan. It could include Cognitive behavioral therapy, Family therapy or group therapy.
Psychoeducation
Particularly in bipolar disorder the knowledge about the disease is essential. For patients and caregivers as well. It’s important to identify individual risk factors and triggers and to develop strategies to avoid them. Moreover the patient has to learn to detect early symptoms of another episode.
Lifestyle
The goal is to eliminate all individual risk factors that could trigger a relapse. This could include sleep pattern, substance use, stress at work or in the family. It could be shown that a relapse is less likely if a good sleep pattern is maintained.
Support groups
To have a good psychiatrist and a professional health support is important. However, besides this it is big help to get help from other sufferers or caregivers as well. Here you can find more information about our free of charge support group.
Video
References
- Poolsup N, Li Wan Po A, de Oliveira IR. Systematic overview of treatment in acute mania. J Clin Pharm Ther. 2000;25:139-56
- Macritchie K, Geddes JR, Scott J, et al. V for acute mood episodes in bipolar disorder. Cochrane Database Syst Rev. 2003:CD4052
- Davis JM, Janicak PG, Hogan DM. M in the prevention of recurrent affective disorders: a meta-analysis. Acta Psychiatr Scand. 1999;100:406-17
- Donna Sudak, MD
- Tondo L, Hennen J, Baldessarini RJ. Lower suicide risk with long-term L treatment in major affective illness: a meta-analysis. Acta Psychiatr Scand. 2001;104:163-72
- Geddes JR, Burgess S, Hawton K, et al. Long-term L therapy for bipolar disorder: systematic review and meta-analysis of randomized controlled trials. Am J Psychiatry. 2004;161:217-22
- Goodwin GM, Bowden CL, Calabrese JR, et al. A pooled analysis of 2 placebo-controlled 18-month trials of L and L maintenance in bipolar I disorder. J Clin Psychiatry. 2004;65:432-41
- Macritchie KA, Geddes JR, Scott J, et al. V acid, V and D in the maintenance treatment of bipolar disorder. Cochrane Database Syst Rev. 2001:CD3196
- Ceron-Litvoc D, Soares BG, Geddes J, et al. Comparison of C and L in treatment of bipolar disorder: a systematic review of randomized controlled trials. Hum Psychopharmacol. 2009;24:19-28
- Rendell JM, Gijsman HJ, Keck P, et al. O alone or in combination for acute mania. Cochrane Database Syst Rev. 2003:CD4040
- Yatham LN, Grossman F, Augustyns I, et al. Mood stabilisers plus r or placebo in the treatment of acute mania: international double-blind, randomised controlled trials. [Erratum in Br J Psychiatry 2003;182:369] Br J Psychiatry. 2003;182:141-7
- Rendell JM, Gijsman HJ, Bauer MS, et al. R alone or in combination for acute mania. Cochrane Database Syst Rev. 2006:CD4043
- Lenox RH, Newhouse PA, Creelman WL, Whitaker TM. Adjunctive treatment of manic agitation with L versus H : a double-blind study. J Clin Psychiatry. 1992;53:47-52
- Meehan K, Zhang F, David S, et al. A double-blind, randomized comparison of the efficacy and safety of intramuscular injections of O , L or placebo in treating acutely agitated patients diagnosed with bipolar mania. J Clin Psychopharmacol. 2001;21:389-97
- Gijsman HJ, Geddes JR, Rendell JM, et al. A for bipolar depression: a systematic review of randomized controlled trials. Am J Psychiatry. 2004;161:1537-47
- Nolen WA, Bloemkolk D. Treatment of bipolar depression: a review of the literature and a suggestion for an algorithm. Neuropsychobiology. 2000;42:11-17
- Delbello MP, Schwiers ML, Rosenberg HL, Strakowski SM. A double-blind, randomized, placebo-controlled study of Q as adjunctive treatment for adolescent mania. J Am Acad Child Adolesc Psychiatry. 2002;41:1216-23
- Derry S, Moore RA. Atypical A in bipolar disorder: systematic review of randomised trials. BMC Psychiatry. 2007;7:40
- Geddes JR, Calabrese JF, Goodwin GM. L for treatment of bipolar depression: independent meta-analysis and meta-regression of individual patient data from five randomised trials. Brit J Psychiatry. 2009:194:4-9
- Scott J, Garland A, Moorhead S. A pilot study of cognitive therapy in bipolar disorders. Psychol Med. 2001;31:459-67
- Beynon S, Soares-Weiser K, Woolacott N, et al. Psychosocial interventions for the prevention of relapse in bipolar disorder: a systematic review of controlled trials. Brit J Psychiatry 2008;192:5-11
- Miklowitz DJ, George EL, Richards JA, et al. A randomized study of family-focused psychoeducation and pharmacotherapy in the outpatient management of bipolar disorder. Arch Gen Psychiatry. 2003;60:904-12
- Rea MM, Tompson MC, Miklowitz DJ, et al. Family-focused treatment versus individual treatment for bipolar disorder: results of a randomized clinical trial. J Consult Clin Psychol. 2003;71:482-92
- Colom F, Vieta E, Martinez-Aran A, et al. A randomized trial on the efficacy of group psychoeducation in the prophylaxis of recurrences in bipolar patients whose disease is in remission. Arch Gen Psychiatry 2003;60:402-7
- Perry A, Tarrier N, Morriss R, et al. Randomised controlled trial of efficacy of teaching patients with bipolar disorder to identify early symptoms of relapse and obtain treatment. BMJ 1999;318:749-63
Schizophrenia
What is Schizophrenia?
Schizophrenia is a brain disorder. It affects the way a person acts, thinks and sees the world. Often people with schizophrenia have different perception of reality and even lose contact with reality. They might see things, that others do not see or might hear voices that others do not hear (hallucinations). They might even speak in a confusing way or might believe in their own „reality“(delusion). Even some people feel persecuted or constantly watched (paranoia). Others have a disorganized behaviour or so-called „negative symptoms“, such as lack of emotional expressions or lack of enthusiasm. If a person shows symptoms as a radical change in personality and an impaired functioning plus a distorted or non-existent sense of reality we speak in medical terms of „psychosis“.
Schizophrenia typically begins in the early adulthood, between the age of 15 and 25. Women tend to develop first symptoms several years later than men, typically around the age of 25. However, men are more affected than women. Symptoms might develop slowly or sometimes it shows the full syndrome immediately. Early warning signs of schizophrenia could be a social withdrawal, depression, suspiciousness or inappropriate laugh or crying. It is important to be aware of early symptoms, because the earlier the disorder is diagnosed the better it can be treated.
Schizophrenia is affecting approximately 0.7 to 1.0 percent of the adult population worldwide. About 26 million people worldwide are affected by schizophrenia. We would therefore estimate to have about 50'000 people suffering from schizophrenia in the UAE.
While schizophrenia is among the common mental disorders, anxiety and mood disorders such as depression are 5 to 10 times more frequent. In the past years there was a longstanding opinion that the prevalence of schizophrenia varied little from population to population. Today we have indications that the rates of schizophrenia can vary in different regions due to the influence of cultural, urban and geographic factors. For example migrants have higher prevalence’s then native-born individuals and developed countries higher prevalence’s then non-developed countries. The highest prevalence is among people with low socioeconomic status living in developing nations. Recent studies suggest that environmental factors related to urban residence may contribute to development of schizophrenia.
The WHO published data 2002 regarding the prevalence of schizophrenia and we know, that the disorder tends to be the highest in Oceania and Middle East and Asia compared to Australia, Japan and Europe.
Symptoms and Signs
 There are two kinds of symptoms – early symptoms which may exist years before the actual outbreak of Schizophrenia - and main symptoms. The early symptoms include the alteration of experience and conspicuousness in conduct although to a small extent that it will not easily be brought into connection with early signs of schizophrenia.
There are two kinds of symptoms – early symptoms which may exist years before the actual outbreak of Schizophrenia - and main symptoms. The early symptoms include the alteration of experience and conspicuousness in conduct although to a small extent that it will not easily be brought into connection with early signs of schizophrenia.The main symptoms of Schizophrenia are Delusions, Hallucinations, disorganized speech, disorganized behavior and negative symptoms like diminished emotional expression or avolition. These symptoms mark the active phase of the disorder which emerges after a stressor or substance abuse or without any identifiable stressor. Patients often suffer from social disorders due to a loss of personal abilities such as initiative, interest, and pleasure in life and other people. Their emotions may be blunted and there may be a poverty of speech and diminished activity and self-care. Moreover Schizophrenia often affects cognitive areas such as memory and attention. A lack of decision-making capability is common, especially in older patients.
Causes
Today the causes of schizophrenia are not fully known. It appears to be a result of a complex interaction between genetic (hereditary) and environmental factors. Schizophrenia has a strong hereditary component, which means, that individuals with a first-degree relative who has schizophrenia have a 10 percent chance to develop the disorder, so an approximately 15 times higher risk than the average population.
But it is important to mention, that the disorder is only influenced, not determined by genetics. So we know that the inherited genes make a person vulnerable to get schizophrenia, but the environmental factors act on the vulnerability and trigger the onset of the disorder. From research we know, that „stress-inducing“factors might be involved in schizophrenia, such as prolonged birth, malnutrition before birth or prenatal exposure to a viral infection. Problems with certain naturally occurring brain chemicals, including neurotransmitters called dopamine and glutamate, also may contribute to schizophrenia. Neuroimaging studies show differences in the brain structure and central nervous system of people with schizophrenia.
Stigma
In many cultures mental health is a theme that is not openly discussed and even stigmatized. We would help many patients when we could overcome being „speechless “and support them to seek for professional help. This would be the first step to get a treatment and improve the quality of life for the patients and their families. An obstacle for many patients with early symptoms is also that mental disorders are often poorly covered by health insurances resulting in further delays of diagnosis and treatment.
Diagnosis
Schizophrenia is a clinical diagnosis. Certain tests will be ordered to rule out other illnesses and conditions that may trigger schizophrenia-like symptoms. The tests may include a complete blood count, urinalysis, a metabolic profile, imaging studies and psychological evaluation. Best Psychologist in Dubai will assess the patient's mental state by asking about thoughts, moods, hallucinations, suicidal traits, violent tendencies or potential for violence, as well as observing their demeanor and appearance. Patients with suspected schizophrenia should be referred for a psychiatric assessment. At least one of the symptoms must be delusions, hallucinations or disorganized speech.
If you're unable to know what your mental health concern is, we can help you with that using our best Neurologist in Dubai, Psychiatrist in Dubai, and Psychologist in Dubai's help.
Treatment of Schizophrenia
Schizophrenia can be treated and the outlook for the disorder continues to improve. However, only 50% of patients receive adequate help. Very often people under appropriate and continuous treatment can live a regular life and work. It should be treated with a complex setting that includes medication, psychotherapy and the establishment of a strong support network. Unfortunately, many patients do not receive the appropriate treatment today because of a lack of social acceptance and/or the inability to recognize the need for treatment by the patients themselves.
An effective treatment requires a combination of medication and psychotherapy. Treatment helps relieve many symptoms of schizophrenia, but most people who have the disorder cope with symptoms throughout their lives and most will remain on antipsychotics for the rest of their lives. Nevertheless, antipsychotics should not be used as a single-treatment modality. Therapy and psychosocial interventions should continue.
Psychosocial treatments help patients deal with the everyday challenges of the illness. Learning and using coping mechanisms to address these problems allow people with schizophrenia to socialize and attend school and work. Support Groups can be an effective adjunct to medication as well and help patients reach out to others facing similar challenges. Support groups may also help family and friends cope.
However, many people with schizophrenia can lead rewarding and meaningful lives.
© GNC, German Neuroscience Center Dubai (Neurology, Psychiatry, Psychology, Counseling, Dubai, UAE)
PTSD – Post Traumatic Stress Disorder
Disease
PTSD: Post Traumatic Stress Disorder Symptoms, Treatment & More
.
What is Post traumatic stress disorder (PTSD)?
Post-traumatic stress disorder - PTSD - is a serious mental health condition that occurs after a traumatic event. PTSD is a lasting consequence of traumatic ordeals that cause intense fear, helplessness, or horror. It could remain for month or even years. It could start directly after the event or delayed by months. After experiencing or witnessing a terrifying event a person may have difficulties coping and adjusting it. The person may feel stressed or frightened even when he is no longer in danger. These feelings continue and even increase, becoming so strong that they keep the person from living a normal life.
Symptoms
Post-traumatic stress disorder (PTSD) could include many symptoms. Most often they begin within three month of the traumatic event. There are three main categories of PTSD Symptoms:
- Reliving: The person with post-traumatic stress disorder repeatedly relives the traumatic event as if it were happening again. This may include flashbacks, nightmares and hallucinations. He or she also may feel severe emotional distress or physical reactions to something that reminds him of the event.
- Avoiding: The person avoids thinking or talking about the traumatic event. He or she may also avoid places, events or objects that reminds him or her of the trauma which can lead to feelings of detachment and isolation. A strong guilty feeling and depression may occur.
- Increased arousal: The person may feel tense, frightened and easily startled. He or she may experience troubles of sleeping and concentrating as well as irritability or outbursts of anger. Physical symptoms, such as increased blood pressure and heart rate, rapid breathing, muscle tension, nausea, and diarrhea also may occur.
Moreover the person could feel depressed or emotional numb. Sometimes the patients block the event completely from their memory.
Causes
A person suffering from PTSD can develop a post-traumatic stress disorder when he or she goes through or witnesses a traumatic event, such as sexual violation, torture, child abuse, car accidents, sudden death of a loved one or a natural disaster. PTSD can occur in anyone who has experienced a traumatic event but it is assumed that it is caused by a mix of the brain regulation of stress chemicals and hormones and inherited mental health risks, such as an increased risk of anxiety and depression. Moreover, life experiences and inherited aspects of the personality do play a big role.
If you're unable to know what your mental health concern is, we can help you with that using our top Neurology Doctor, Psychiatry Doctor, and Psychology doctor's help.
Treatment
The treatment of PTSD is very effective. The goal is to support the coping skills of the patient to be able to deal with the traumatic event. The main treatments for people with post-traumatic stress disorder are psychotherapy or medications, sometimes both. The patient will learn certain skills to address the symptoms and thus improve the symptoms. The Psychologist helps in coping if any symptoms arise again.
Cognitive behavioral therapy (CBT) is a very helpful therapy when suffering from PTSD. There are several parts to CBT, including:
- Exposure therapy: It helps facing and controlling the fear by mental imagery, writing, or visiting the place where the event happened.
- Cognitive restructuring: It helps recognizing the way of thinking such as negative or inaccurate ways of perceiving normal situations. Sometimes people remember the event differently than how it happened. The Psychologist helps looking at things in a realistic way.
- Stress inoculation training: It helps reducing the symptoms by reducing anxiety. It helps looking at the memories in a healthy and realistic way.
All these approaches can help reducing fear after a traumatic event. The best type of treatment should be discussed individually with the Psychologist. Moreover, certain medications, such as Antidepressants and Anti-anxiety medications, can improve the feelings of anxiety and stress. Sometimes a combination of psychotherapy and medications is recommended by the Specialist.
Furthermore the PTSD patient will learn relaxation techniques such as PMR or autogenic training. It is recommended that the patient visits a support group as well to learn from other sufferers how they managed the situation.
© GNC, German Neuroscience Center Dubai (Neurology, Psychiatry, Psychology, Counseling, Dubai, UAE)
Acute reaction to Stress
Disease
Stress Disorders in Dubai: Understanding and Managing Acute Stress Reactions
Are you feeling overwhelmed, unable to cope with everyday life events, or experiencing persistent distress after a traumatic incident? You may be suffering from an acute stress disorder. At German Neuroscience Center, we specialize in providing professional help and support for individuals in Dubai who are facing stress disorders. Our dedicated team of experts is here to guide you towards a healthier, more balanced life.
Acute stress disorders can arise from extreme life events that disrupt our sense of stability and security. These events may include the loss of a loved one, experiences of violence, separation, accidents, trauma, or abuse. Sometimes, even seemingly simple occurrences like attending school or relocating can trigger a stress reaction. It is natural to feel sadness, shock, or confusion when faced with such events.
However, if your reaction persists for an extended period, becomes unmanageable, or seems disproportionate to the event itself, seeking professional help is crucial. The impact of stress disorders can manifest in various ways, such as restricted consciousness, decreased attention, disorientation, amnesia, depression, desperation, anxiety, aggression, and even physical symptoms like sweating, rapid heartbeat, and blushing.
When an acute reaction to stress occurs immediately after an event and gradually subsides, it is considered a normal response. Nonetheless, depending on the intensity of the symptoms, it may be necessary to seek professional assistance for a short period to regain control over your life.
At German Neuroscience Center, we understand the unique challenges faced by individuals in Dubai. Our team of experienced professionals specializes in stress disorders, providing comprehensive evaluations and tailored treatment plans to address your specific needs. We employ evidence-based therapeutic approaches to help you develop effective coping mechanisms, regain emotional well-being, and restore balance in your life.
Our clinic offers a welcoming and supportive environment where you can openly discuss your experiences and concerns. We prioritize your mental health and are committed to guiding you towards a brighter, healthier future. Our team utilizes a holistic approach, combining therapy, counseling, and other proven interventions to address the root causes of your stress disorders.
When you choose German Neuroscience Center, you are selecting a trusted partner dedicated to your well-being. Our expert therapists are equipped with the knowledge and experience to navigate the complexities of stress disorders, providing you with the tools necessary to overcome challenges and regain control over your life.
Don't let stress disorders hinder your happiness and quality of life. Take the first step towards healing by seeking professional help at German Neuroscience Center. Contact us today to schedule an appointment and embark on your journey to a stress-free, fulfilling life.
Remember, you don't have to face stress disorders alone. At German Neuroscience Center, we are here for you every step of the way.
Book your appointment today and start your journey towards a healthier, happier you. Let us be your partner in overcoming stress disorders in Dubai.
Abuse Treatment & Recovery in Dubai | German Neuroscience Centre
Abuse is a deeply concerning issue that affects individuals physically, emotionally, and psychologically. Recognizing the signs, understanding risk factors, and seeking effective treatment are vital steps towards breaking free from its grip. The German Neuroscience Center Dubai stands as a beacon of hope, offering specialized care and a multidisciplinary approach to help victims overcome abuse and reclaim their lives.Signs and Symptoms of Abuse
Abuse can manifest in various forms, leaving distinct signs and symptoms in its wake. Victims may experience unexplained injuries, frequent absences from work or social engagements, sudden changes in behavior, anxiety, depression, withdrawal, and low self-esteem. At the German Neuroscience Center Dubai, our experts are trained to recognize these signs and provide empathetic support.Risk Factors of Abuse
Certain factors can increase the likelihood of experiencing abuse. These include a history of trauma, low self-esteem, lack of social support, substance abuse, and dependence on the abuser. Recognizing these risk factors is essential for early intervention. The German Neuroscience Center's team is experienced in tailoring interventions to address individual risk factors.Causes of Abuse
Abuse can stem from a variety of underlying causes, including power dynamics, unresolved trauma, mental health issues, and learned behaviors. Understanding these root causes is crucial for creating effective treatment plans. Our clinicians at the German Neuroscience Center Dubai delve deep into the individual's history to identify these causes and devise personalized therapeutic strategies.Forms of Abuse
Abuse takes on various forms, each with its own devastating impact. This includes physical abuse, emotional and psychological abuse, sexual abuse, financial abuse, and neglect. Victims may experience a combination of these forms, leading to complex psychological distress. The German Neuroscience Center Dubai offers a comprehensive approach that addresses the multidimensional effects of abuse.Diagnostics
Accurate diagnosis is the cornerstone of effective treatment. Our specialists at the German Neuroscience Center Dubai employ a range of diagnostic tools, including comprehensive psychological assessments, interviews, and medical examinations. These assessments provide a holistic view of the individual's physical and psychological health, guiding the development of a tailored treatment plan.Treatments of Abuse
Recovery from abuse requires a multifaceted approach that integrates medical, psychological, and support interventions. The German Neuroscience Center Dubai's team of experts collaborates to create personalized treatment plans that may include psychotherapy, counseling, medication, support groups, and holistic therapies. Our commitment to holistic healing ensures that every aspect of a patient's well-being is addressed.Therapeutic Modalities
At the German Neuroscience Center Dubai, a range of evidence-based therapeutic modalities are employed to facilitate healing. Cognitive-behavioral therapy (CBT), trauma-focused therapy, dialectical behavior therapy (DBT), and art therapy are just a few of the approaches utilized. Our clinicians work closely with patients to determine the most suitable therapies for their unique needs.Support System
Recovering from abuse requires a strong support system. The German Neuroscience Center Dubai offers a safe and nurturing environment where patients can share their experiences, connect with others facing similar challenges, and access resources for ongoing healing. Our compassionate team is dedicated to empowering individuals to rebuild their lives.Conclusion
Abuse is a formidable adversary, but with the right resources and support, victims can overcome its grip and regain control of their lives. The German Neuroscience Center Dubai stands as a beacon of hope, offering comprehensive care that addresses the physical, emotional, and psychological aspects of abuse. Our experienced team is committed to guiding patients towards a path of healing, recovery, and empowerment. If you or a loved one are seeking help, reach out to the German Neuroscience Center Dubai, where compassion and expertise converge to pave the way for a brighter future.Adjustment Disorder
Disease
Adjustment Disorders
Adjustment Disorder means that a normal reaction to stress starts as late as a month after the event and will continue up to six months. This still would be considered a normal reaction although also in these cases therapeutic help might be necessary
© GNC, German Neuroscience Center Dubai (Neurology, Psychiatry, Psychology, Counseling, Dubai, UAE)
Trauma Therapy & PTSD Treatment in Dubai | GNC
Trauma, in its various forms, can have a profound impact on an individual's physical, emotional, and psychological well-being. Whether stemming from accidents, violence, or other distressing events, trauma can lead to a range of symptoms that may affect a person's quality of life. The German Neuroscience Center (GNC) in Dubai stands as a beacon of hope and healing, offering cutting-edge treatments and compassionate care to help individuals overcome trauma and embark on a journey towards recovery.Signs and Symptoms of Trauma
Trauma can manifest in a multitude of ways, with symptoms varying depending on the severity and nature of the traumatic event. Common signs of trauma include:- Re-experiencing: Flashbacks, nightmares, and intrusive thoughts about the traumatic event.
- Avoidance: Avoidance of triggers associated with the trauma, leading to withdrawal from people, places, or activities.
- Hyperarousal: Heightened alertness, irritability, difficulty concentrating, and an exaggerated startle response.
- Emotional Disturbances: Intense feelings of guilt, shame, anger, and sadness that may persist long after the event.
- Physical Symptoms: Headaches, muscle tension, fatigue, and disrupted sleep patterns.
Risk Factors for Trauma
Certain factors can increase an individual's vulnerability to experiencing trauma. These risk factors include:- Previous Trauma: A history of prior traumatic experiences can make individuals more susceptible to subsequent trauma.
- Lack of Support: Limited social support systems and isolation can magnify the impact of trauma.
- Personal Resilience: Some individuals may possess greater resilience, allowing them to cope more effectively with traumatic events.
- Exposure to Violence: Frequent exposure to violence, either as a victim or witness, can heighten the risk of trauma.
- Preexisting Mental Health Conditions: Individuals with preexisting anxiety, depression, or other mental health disorders may be more prone to trauma-related effects.
Causes and Diagnostics of Trauma
Trauma can arise from a range of events, such as accidents, natural disasters, interpersonal violence, and medical procedures. Diagnosing trauma involves a comprehensive assessment that considers the patient's history, symptoms, and emotional responses. The experienced clinicians at GNC employ state-of-the-art diagnostic techniques, including psychological evaluations and neuroimaging, to accurately assess the impact of trauma on an individual's mental and physical health.Trauma Treatments at German Neuroscience Center Dubai
The German Neuroscience Center in Dubai is renowned for its holistic approach to trauma treatment, offering a wide array of evidence-based interventions tailored to the unique needs of each patient. These include:- Psychotherapy: Individual and group therapies such as Cognitive Behavioral Therapy (CBT) and Eye Movement Desensitization and Reprocessing (EMDR) to address trauma-related symptoms and promote healing.
- Medication: In cases where symptoms are severe, targeted medications can be prescribed to alleviate anxiety, depression, and other distressing symptoms.
- Mind-Body Techniques: Practices like yoga, meditation, and deep breathing can help regulate the body's stress response and promote emotional well-being.
- Neurofeedback: Cutting-edge neurofeedback techniques aim to retrain brain patterns, facilitating emotional regulation and symptom reduction.
- Art and Expressive Therapies: Creative outlets can provide a means of processing trauma when words fall short.
Why Choose German Neuroscience Center Dubai?
The German Neuroscience Center Dubai stands as a beacon of hope and healing for individuals seeking comprehensive trauma treatment. With a team of internationally renowned experts, advanced diagnostic tools, and a patient-centric approach, GNC offers a safe and supportive environment for those on their journey to recovery. The center's commitment to excellence, innovation, and personalized care sets it apart as the premier destination for trauma treatment in the region.Conclusion
Trauma's effects can be far-reaching, impacting every facet of an individual's life. However, with the comprehensive and compassionate care provided by the German Neuroscience Center Dubai, healing is within reach. From cutting-edge treatments to a commitment to patient well-being, GNC stands as a beacon of hope, guiding individuals towards a brighter future where trauma's grip is loosened, and life's joys can once again be embracedSomatoform disorder
Somatoform Disorders
 Somatoform disorders are defined as somatic (bodily) symptoms without a sufficient somatic (bodily) cause. Only after somatic causes are ruled out, psychological factors can be taken into consideration. The presentation of the symptoms is the same, regardless if they are caused by somatic or psychological factors. A good example is common back pain. It can be caused by a pinched nerve as a somatic cause. The exact same pain can be cause by psychological factors, too. For most people this seems to be hard to believe. However, somatoform disorders are among the most common psychiatric disorders and occur in 10 to 15% of primary care patients.
Somatoform disorders are defined as somatic (bodily) symptoms without a sufficient somatic (bodily) cause. Only after somatic causes are ruled out, psychological factors can be taken into consideration. The presentation of the symptoms is the same, regardless if they are caused by somatic or psychological factors. A good example is common back pain. It can be caused by a pinched nerve as a somatic cause. The exact same pain can be cause by psychological factors, too. For most people this seems to be hard to believe. However, somatoform disorders are among the most common psychiatric disorders and occur in 10 to 15% of primary care patients.Somatoform disorders can cause almost all kind of symptoms. From pain over irritable bowel syndrome up to the fear of a brain tumor. As it is very natural to believe in a somatic reason, patients tent to undergo various medical investigations – even unnecessary surgeries. Sometimes patients are searching for a reason that explains the symptoms for years. They are consulting doctors frequently, which is called “doctor hopping” and often turn to alternative medicine. This kind of behavior expresses the enormous pressure these patients are under.
It is important to understand that these patients are ill, they will have pains, functional disorders or likewise. People with somatoform disorders are not faking their symptoms and their symptoms can significantly affect daily functioning. Their pain often has a dramatic impact of work, relationships, and other activities.
Types and Symptoms
1. Somatization disorder / Somatic Symptom Disorder
This type of somatoform disorder includes symptoms such as pain, neurologic problems, sexual problems, gynecological, cardiologic and gastrointestinal complaints. Patients often have a long history of medical problems but never a diagnosis that could really explain all their symptoms.
2. Undifferentiated somatoform disorder
One speaks of an undifferentiated somatoform disorder if the patient has one or more physical complaints of unexplained symptoms for at least six months.
3. Hypochondriasis
If a patient is concerned about having a serious disease and believes that minor complaints are signs of very serious medical problems he is suffering from this type of somatoform disorders.
4. Conversion disorder
In this type the patient has neurological symptoms such as paralysis, blindness, hearing loss or a loss of sensation or numbness without any medical cause.
5. Pain disorder
Patients with pain disorder typically experience pain that started with a psychological stress or trauma such as chronic headache after a stressful life event.
Diagnosis
Finding the diagnosis can be difficult and time consuming. A comprehensive medical examination including laboratory work and radiologic scans is needed to determine possible causes of the symptoms. It is very important to not overlook any somatic (bodily) cause. On the other side the patient shall be protected from unnecessary medical investigations and surgeries. If the examination does not reveal a clear source of the pain a somatoform disorder could be considered.
If you're unable to know what your mental health concern is, we can help you with that using our top Neurology Doctor, Psychiatry Doctor, and Psychology doctor's help.
Treatment
A strong doctor-patient relationship plays a key role in the effective treatment of somatoform disorders. For the patient it is important to understand that treating a somatoform disorder doesn’t mean neglecting the possibility of a somatic cause. It is not an either or decision the patient has to make. Treating a somatoform disorder correctly is rather an addition to the attempts the patient did so far. The doctor will evaluate all performed procedures and decide with the patient which further investigations are necessary and which ones are not. Patient and doctor together will develop a concept that takes all factors influencing the disease in consideration. These factors can be very different from patient to patient. Depending on this, different forms of treatment are effective. Cognitive behavioral therapy is used since it focuses on correcting distorted thoughts, unrealistic beliefs and behaviors that prompt health anxiety. The focus is rather on the improvement of daily functioning then on managing symptoms. Stress reduction is often an important part of getting better. Antidepressant medications can support the psychotherapy. Moreover, Support Groups can be helpful as well as stress reduction exercises, physical therapy and massage. The doctor will develop an individual treatment plan for each patient.
Obsessive-Compulsive Disorder (OCD)
Obsessive-Compulsive Disorder (OCD) is a complex mental health condition that affects millions of people worldwide. Characterized by persistent and distressing thoughts (obsessions) and repetitive behaviors (compulsions), OCD can significantly disrupt an individual's daily life, causing distress and anxiety. If you or a loved one is struggling with OCD, rest assured that the German Neuroscience Center in Dubai is dedicated to providing comprehensive and specialized care to help you overcome these challenges.Symptoms of Obsessive-Compulsive Disorder (OCD)
OCD manifests through a wide range of symptoms, often involving intrusive thoughts and the need to perform certain behaviors to alleviate anxiety. Common obsessions include fear of contamination, concerns about harming oneself or others, and an overwhelming need for symmetry and order. Compulsions, on the other hand, might involve repetitive actions like washing hands, checking locks, or counting objects to neutralize the distress caused by the obsessions.Risk Factors for Obsessive-Compulsive Disorder (OCD)
While the exact cause of OCD remains unclear, several risk factors have been identified:- Genetics: Family history of OCD can increase the likelihood of developing the disorder.
- Brain Structure and Function: Certain brain abnormalities or imbalances in neurotransmitters may contribute to OCD.
- Trauma: Childhood trauma or significant life stressors can trigger the onset of OCD in susceptible individuals.
- Personality Traits: Perfectionism, high levels of anxiety, and a propensity for excessive worry can increase vulnerability.
Causes of Obsessive-Compulsive Disorder (OCD)
The development of OCD is likely influenced by a combination of genetic, neurological, and environmental factors. Research suggests that an interplay between genetic predisposition and brain chemistry plays a crucial role. Abnormalities in the brain's circuitry involving the basal ganglia and frontal cortex are thought to contribute to the disorder's symptoms.Diagnosis of Obsessive-Compulsive Disorder (OCD)
Diagnosing OCD involves a thorough assessment of an individual's symptoms and their impact on daily functioning. A skilled mental health professional at German Neuroscience Center Dubai will conduct a comprehensive evaluation, which may include interviews, psychological questionnaires, and discussions about the history and duration of symptoms. This meticulous process ensures an accurate diagnosis and a personalized treatment plan.Treatments for Obsessive-Compulsive Disorder (OCD)
Effective OCD management often requires a combination of therapy and medication. A Psychiatrist in Dubai can tailor a treatment plan, incorporating Cognitive Behavioral Therapy (CBT), medications, and advanced techniques like dTMS. At German Neuroscience Center Dubai, a multidisciplinary approach is employed to provide the most effective treatments for OCD:- Cognitive-Behavioral Therapy (CBT): CBT, particularly Exposure and Response Prevention (ERP), is a gold-standard psychotherapy for OCD. It involves gradual exposure to feared situations or thoughts and learning healthier ways to manage anxiety without resorting to compulsions.
- Medication: Selective Serotonin Reuptake Inhibitors (SSRIs) are commonly prescribed to manage OCD symptoms. These medications help regulate neurotransmitter levels in the brain and can be especially beneficial when combined with therapy.
- Deep Transcranial Magnetic Stimulation (dTMS): This innovative non-invasive procedure utilizes magnetic fields to stimulate specific brain areas, helping to modulate neural circuits associated with OCD symptoms.
- Support Groups and Education: Engaging in support groups and receiving education about OCD can help individuals and their families better understand the disorder and cope effectively.
Why Choose German Neuroscience Center Dubai for OCD Treatment
German Neuroscience Center Dubai stands out as a leading institution for OCD treatment due to its commitment to providing patient-centered care:- Expertise: The center boasts a team of experienced psychiatrists, psychologists, and therapists with a deep understanding of OCD and its complexities.
- Tailored Treatment Plans: Each patient receives a personalized treatment plan based on their unique needs and preferences, ensuring the highest chances of success.
- Cutting-Edge Therapies: The center offers a wide range of evidence-based treatments, including CBT, medication, and advanced therapies like dTMS.
- Holistic Approach: The team at German Neuroscience Center Dubai recognizes the importance of addressing both the psychological and emotional aspects of OCD, promoting overall well-being.
Conclusion
Obsessive-Compulsive Disorder can be a challenging condition to manage, but with the right support and treatment, individuals can regain control over their lives. German Neuroscience Center Dubai is dedicated to providing the highest quality care for individuals struggling with OCD. Through a combination of expert knowledge, personalized treatment plans, and advanced therapies, the center is committed to helping patients overcome the grip of OCD and embrace a healthier, more fulfilling life.Dissociative Disorder (Conversions)
Disease
Dissociative Disorder (Conversions)
Definition of Dissociative Disorder
Traumatic events or seemingly unsolvable problems can lead to psychic reaction known as dissociative disorder. It is characterized by a disconnection and lack of continuity between thoughts, memories, surroundings, actions and identity. People with a dissociative disorder experience their body or the world around them as unreal and they are uncertain about who they are. They could feel like having many different identities which often leads to problems with functioning in everyday life. They may escape reality in ways that are involuntary and unhealthy.
Symptoms
Signs and symptoms of dissociative disorder could include memory loss (amnesia) of certain time periods, events and people, an inability to recall key personal information that is too far-reaching to be explained as mere forgetfulness, a sense of being detached from yourself and a blurred sense of identity. Along with the dissociation and multiple or split personalities people may also experience depression, mood swings, sleep disorder, anxiety, panic attacks, eating disorders and more.
Dissociative disorder is separated into three major disorders:
1. Dissociative amnesia: People with this disorder are blocking out critical personal information, usually of a traumatic or stressful nature. They can't recall information about themselves or events and people in their life, especially from a traumatic time. These gaps in memory are much more severe than normal forgetfulness, and are not the result of an underlying medical condition.
2. Dissociative identity disorder: This disorder is characterized by alternate identities. People may feel the presence of one or more other people talking or living inside their head and a feeling as though they are possessed by other identities. This disorder was formerly known as multiple personality disorder and it is the most famous of the dissociative disorders. People with dissociative identity disorder typically also have dissociative amnesia and often have dissociative fugue.
3. Depersonalization-derealization disorder: People with this disorder experience a feeling of being outside themselves. They observe their actions, feelings and thoughts from a distance as though watching a movie. A person with depersonalization disorder has this experience so frequently and so severely that it interrupts his or her functioning and experience.
Causes
The main causes for dissociative disorder are traumatic events in the past such as physical, sexual or emotional abuse suffered during childhood, although some people 'dissociate' after experiencing war, kidnapping or even an invasive medical procedure. Switching off from reality is a normal defense mechanism to cope during a traumatic time but it becomes dysfunctional when the environment is no longer traumatic but the person still acts and lives as if it is.
Treatment
The primary treatment for dissociative disorder is psychotherapy. The psychotherapist consultation will help the patient to understand the cause of the condition and to form new ways of coping with stressful circumstances. A person with dissociative disorder might also benefit from drugs such as antidepressants or antianxiety medication. These medications can help to control the mental health symptoms associated with dissociative disorders.
© GNC, German Neuroscience Center Dubai (Neurology, Psychiatry, Psychology, Counseling, Dubai, UAE)


















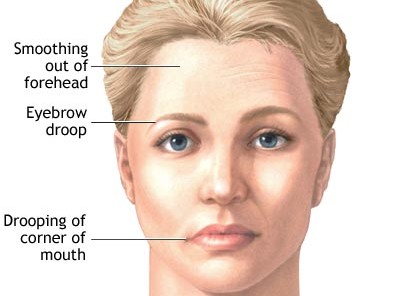
































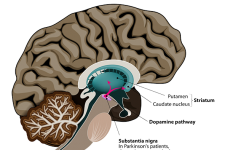





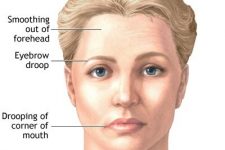


















The German Neuroscience Center Dubai presents a selection of the most common diseases in neurology and psychiatry. At the top you will find a filter for neurological and psychiatric / psychological diseases. By clicking you can filter diseases only in the field of Neurology or Psychiatry / Psychology. Clicking on the pictures will guide you to more information about the specific disease like stroke, epilepsy, multiple sclerosis, parkinsons disease, polyneuropathy, back pain, nerve damage, carpal tunnel syndrome, migraine headache, vertigo, myasthenia gravis, palsy, restless legs syndrome, tremor, trigeminal neuralgia, visual disturbances, dementia, schizophrenia, depression, mania, bipolar, anxiety phobia panick attacks, obsessive compulsive disorder , acute stress, post traumatic stress, adjustment disorders, somatoform disorder, dissociative disorder, eating disorder, sleep disorder, adhd, autism and treatment options in Dubai UAE.
© GNC, German Neuroscience Center Dubai (Neurology, Psychiatry, Psychology, Counseling, Dubai, UAE)
German Neuroscience Center © Copyright
