الأمراض
الصداع النصفي \ الصداع
- المرض
الصداع النصفي
هل تعاني من الصداع؟ لست وحدك! الصداع مرض واسع الانتشار وأحد أكثر الأسباب شيوعًا لزيارة طبيب الأعصاب في دبي. وهو يحدث بأنواع مختلفة وبقوى مختلفة ويمكن أن يضعف جودة الحياة بشكل كبير. من الممكن القيام بشيء ما ضده. ولكن قبل البدء في العلاج، يجب معرفة السبب ويجب إجراء التشخيص الصحيح قبل البدء في العلاج.
أنواع الصداع
هناك العديد من أنواع الصداع. وأكثرها شيوعًا هو الصداع الأساسي مثل الصداع النصفي أو صداع التوتر أو الصداع العنقودي أو الصداع المسكن. يجب أن يعرف طبيب الأعصاب الخاص بك كيف تشعر بالصداع، ومن أين يبدأ؛ وما إذا كانت هناك أعراض مصاحبة له، وما هي مدة استمراره وعدد مرات حدوثه. ثم سيقوم بإجراء فحوصات طبية مختلفة. بعد أن يعرف التشخيص يمكنه أن يعطيك نصيحة للعلاج المناسب. العلاج ممكن!
الصداع النصفي
الصداع النصفي هو أحد أكثر الأمراض العصبية شيوعاً. يعاني حوالي 10 في المئة من البالغين حول العالم من الصداع النصفي، وتزيد نسبة النساء عن الرجال. ويفترض أطباء الأعصاب أن الاختلاف بين الجنسين له على الأرجح أسباب هرمونية ووراثية. يبدأ عادةً في مرحلة المراهقة. بعد السنة الخمسين ينخفض التكرار مرة أخرى.
تتراوح مدة نوبة الألم بين 4 إلى 72 ساعة. يختلف التكرار بين مرة واحدة في السنة إلى مرتين في الأسبوع. يكون الألم معتدلاً إلى عنيف جداً. تكون السمة في الغالب نابضة وعلى جانب واحد فقط من الجمجمة؛ ولكن في بعض المرضى على كلا الجانبين أيضاً. يتأثر أحد الجانبين أكثر من الآخر. في كثير من الأحيان يعاني المرضى من أعراض مصاحبة مثل الغثيان والقيء ومشاكل بصرية وحساسية شديدة ضد الضوء والضوضاء والرائحة. عند ممارسة التمارين البدنية يزداد الألم.
تستمر نوبة الصداع النصفي النموذجية على 4 مراحل. خلال الفترة التمهيدية لا توجد آلام بعد. قد تكون هناك ردود فعل اكتئابية وتهيج وهياج. من المهم أيضاً إبلاغ طبيب الأعصاب عن مثل هذه الأحاسيس؛ حتى لو كنت تعتقد أنه لا علاقة لها بالألم نفسه. قد يقل التركيز؛ وقد يشعر الناس بالتعب ويضطرون إلى التثاؤب كثيراً. قد تحدث الوذمة أو الإمساك أو الرغبة الشديدة في تناول الطعام الحلو أو الدهني. المرحلة الثانية قد تكون هالة. وغالباً ما تكون هناك مشاكل بصرية مع وجود أورام متلألئة أو رؤية مزدوجة. ولكن قد تكون أيضاً اضطرابات في الإحساس أو مشاكل في الحركة والكلام. تستمر الهالة من بضع دقائق إلى ساعة واحدة.
المرحلة الثالثة يسميها أطباء الأعصاب مرحلة الصداع. يبدأ الألم النابض غالباً في الرقبة وينتشر في مؤخرة الرأس ويستقر خلف العين أو عند الصدغ. وتكون معظم النوبات مصحوبة بأعراض نباتية. يتأثر الجسم كله. بعض الناس غير قادرين على مواصلة عملهم. يضطرون إلى الاستلقاء. يبحثون عن الهدوء والظلام، ولا يرغبون في سماع أو رؤية أي شيء أو أي شخص. قد تصل مدة الصداع إلى 3 أيام إذا لم تنقطع النوبة بالأدوية. بعد ساعات أو من يوم إلى يومين من نوبة الصداع النصفي (المرحلة الرابعة) يشعر الأشخاص بالتعب والإرهاق، ويظل التركيز منخفضًا، وقد يكون المزاج متأرجحًا.
الأسباب
وهو خلل وظيفي مؤقت في الدماغ. أثناء نوبة الصداع النصفي تتسع الأوعية الدموية للغشاء الدماغي وتلتهب. تتهيج الألياف العصبية حول الأوعية بشدة بحيث ترسل إشارات الألم.
هناك محفزات مختلفة للصداع النصفي مثل الإجهاد، والحيض، والكحول، وخاصة النبيذ الأحمر، واضطرابات في دورة النوم والاستيقاظ، والوجبات غير المنتظمة، وتغيرات الطقس، ومحفزات الضوء، والرائحة أو الألم في الرقبة. هذه المحفزات فردية جداً وتختلف حتى لدى الفرد الواحد من وقت لآخر. لكن هذه المحفزات ليست هي أسباب المرض بل تحفزه فقط.
العلاج
في الوقت الحاضر، يستخدم أطباء الأعصاب خيارات علاجية فعالة وسريعة جداً للصداع النصفي.
إذا كنت تعتقد أن زيارة طبيب الأعصاب قد لا تصلح ما تعاني منه. يقدم لك GNC دبي أحد أفضل الأطباء النفسيين في دبي والأطباء النفسيين في دبي والمعالجين النفسيين في دبي الذين يمكنهم مساعدتك في العثور على السبب الأساسي وفي إصلاحه.
علاج الصداع النصفي بدون دواء:
1. تقليل عوامل التوتر قدر الإمكان- تعلم الإدارة الجيدة للوقت: خطط لجدول يومك. لا تنسى وقتاً كافياً للفرامل.
- تعلّم أن تقول "لا".
- لا تفرط في العمل. لا يجب القيام بكل شيء على الفور.
- فكّر: "لا أحد كامل!"
- خذ الحياة بسهولة واستمتع بها.
- 2. الاسترخاء
تساعد إجراءات الاستجمام مثل اليوغا أو التدريب الذاتي المنشأ أو تقنيات استرخاء العضلات التدريجي ولكن يجب القيام بها بانتظام
3. العلاج النفسي
يمكن أن تظهر الأبحاث أن العلاج السلوكي المعرفي (CBT) له تأثير إيجابي على مرضى الصداع النصفي. حتى أن استشارة المريض قادرة على تقليل تواتر نوبات الصداع النصفي. لذلك تم إدراج العلاج السلوكي المعرفي السلوكي في المبادئ التوجيهية للجمعية الألمانية للصداع والصداع النصفي.
4. رياضات التحمل
تُعد رياضات التحمل مثل ركوب الدراجات أو المشي أو الركض أو السباحة جيدة. ولكن من المهم ممارسة الرياضة بانتظام، على الأقل ثلاث مرات في الأسبوع لمدة 30 دقيقة تقريباً.
5. النوم
دورة النوم والاستيقاظ المستمرة، وكذلك خلال عطلة نهاية الأسبوع. وتناول الطعام والشراب بانتظام.
6. المشغلات
تجنبي محفزات الصداع النصفي لدى أفرادك.
علاج الصداع النصفي بالأدوية
1. علاج نوبات الصداع النصفي الحاد
هناك أنواع مختلفة من الأدوية لعلاج النوبة الحادة. في الحالات الأسهل يمكن أن تكون المسكنات الشائعة كافية. يمكن إعطاؤه مع دواء ضد الغثيان. ولكن في الغالب تكون هناك حاجة إلى أدوية أقوى. يمكن أن تخفف أدوية الصداع النصفي الخاصة من حدة النوبة في غضون ساعتين لدى معظم المرضى. يجب وصف هذا النوع من الأدوية من قبل طبيب أعصاب. يجب تناول الدواء في أقرب وقت ممكن. فهو يساعد بشكل أفضل. ولكن كن حذراً. يجب عدم تناول أي مسكن للألم أكثر من 10-12 مرة في الشهر. وإلا فهناك خطر الإصابة بالصداع المسكن، وهو ما يعني الصداع بسبب الدواء نفسه!
2. الوقاية الطبية من الصداع النصفي
في الحالات الشديدة، من المفيد تناول دواء خاص كل يوم لتقليل عدد النوبات أو طول مدة النوبة الواحدة أو لتحسين تأثير الدواء الحاد. يجب تناول هذا الدواء لمدة ثلاثة أرباع السنة على الأقل، وأحياناً لفترة أطول. سيحدد طبيب الأعصاب الخاص بك الدواء الأفضل لك وسيشرف عليك خلال العلاج.
- المرض
الدوار
المرض
دوار، دوار ودوخة
يعاني ما يقرب من 15% من السكان من الدوخة أو الدوار أو عدم التوازن أو الدوار أو الدوار أو عدم الاتزان. الدوار هو الإحساس بالحركة دون حركة فعلية (وهم الحركة). والأكثر شيوعًا هو الإحساس بالدوران (إما أن تدور الغرفة أو أن الشخص يدور). ولكن يمكن أن يكون الإحساس بالحركة الجانبية أو التمايل أو الميل أيضاً. الدوار هو نوع من الدوخة. ومع ذلك، يمكن أن يشمل الدوار أيضاً أعراضاً أخرى لا تترافق بالضرورة مع الشعور بالدوران، مثل عدم التوازن والدوار والدوخة والدوار وعدم الثبات. الدوار هو عرض وليس تشخيصاً. وهذا يعني أن الدوار يمكن أن يكون ناتجاً عن مجموعة واسعة من الأمراض؛ من غير المؤذية إلى المهددة للحياة. نركز في هذه المقالة على الأمراض العصبية الأكثر شيوعاً.
الأعراض والعلامات
يعاني المرضى في أغلب الأحيان من الشعور بالدوار أو الدوار أو عدم التوازن أو الدوخة أو الدوار أو عدم الثبات. علاوة على عدم استقرار الوضعية والشعور بالسقوط أو السقوط الفعلي. غالباً ما يحتاج المرضى إلى الجلوس أو الاستلقاء ويعانون من الغثيان أو القيء. قد يظهر الترنح (صعوبات في المشي) والرأرأة (حركات العين). واعتماداً على السبب الأساسي يمكن أن تظهر الأعراض التالية: فقدان السمع وطنين الأذن وضغط الأذن ومشاكل بصرية. بالإضافة إلى خدر في الجلد، وضعف العضلات، ومشاكل في التنسيق، وصعوبات في الكلام أو اللغة، وصعوبة في البلع.

الأسباب
يمكن أن تكون أسباب الدوار أو الدوخة متعددة. هناك العديد من الأمراض التي يمكن أن تسبب أعراض الدوار. يمكن أن يكون مرضاً في الأذن أو الأذن الداخلية أو العصب الدهليزي أو جذع الدماغ. قد يتطلب الأمر إجراء فحوصات شاملة لمعرفة السبب الحقيقي. نود هنا تسليط الضوء على الأسباب الأكثر شيوعاً.
1.الدوار الموضعي الحميد (BPPV): يُعدّ الدوار الموضعي الحميد السبب الأكثر شيوعًا للدوار. يمكن لبعض حركات الرأس أن تثير نوبة دوار. تكون هذه النوبات قصيرة (أقل من 30 ثانية). وغالبًا ما تحدث نوبة الدوار ليلًا أثناء التقلب في السرير. ينتج هذا النوع من الدوار عن بلورات صغيرة من ترسبات الكالسيوم في قناة الأذن، والتي تتحرك أحيانًا نتيجة أوضاع أو حركات معينة للرأس. وهو شكل شائع جدًا من أنواع الدوار.
- التهاب العصب الدهليزي: يحدث التهاب العصب الدهليزي بسبب التهاب العصب في القنوات نصف الدائرية الذي يساعد على التحكم في التوازن. ويتميز بنوبة شديدة مفاجئة من الدوار تستمر لمدة سبعة إلى عشرة أيام.
- مرض مينير: يتسبب هذا الاضطراب في الأذن الداخلية في حدوث نوبات تلقائية من الدوار إلى جانب فقدان السمع المتذبذب. وغالباً ما يصاحبه طنين (طنين في الأذن) وشعور بالضغط أو الامتلاء في الأذن.
- التهاب التيه: التهاب في بنية الأذن الداخلية التي تسمى المتاهة، وهو التهاب في بنية الأذن الداخلية التي تسمى المتاهة، ناتج عن التهابات بكتيرية في الأذن الوسطى لم يتم علاجها. ويمكن أن يسبب أيضاً فقدان السمع.
- صدمة الرأس: يمكن أن تتسبب الضربة العنيفة على الرأس في تلف الأذن الداخلية. وقد يؤدي ذلك إلى حدوث مشاكل في التوازن مثل الدوار أو الدوخة المؤقتة أو الدائمة.
- أمراض أخرى: الصداع النصفي، متلازمة انسلاخ القناة العلوية، التهاب الأذن الوسطى، الهربس النطاقي الأذني، أمراض القلب وانخفاض ضغط الدم، مرض باركنسون، السكتة الدماغية، ورم الدماغ، ورم الدماغ، ورم العصب السمعي، الورم الشفاني الدهليزي، الصرع، التشوه الخياري، التصلب المتعدد، التصلب المتعدد، الناسور الكوليستيرولي، الناسور حول اللمفاوي، متلازمة انسلاخ القناة نصف الدائرية العلوية، أمراض المناعة الذاتية، الاضطرابات النفسية مثل نوبات الهلع أو القلق
الإجراءات التشخيصية
يجب أن تكون الخطوة الأولى دائمًا استشارة الطبيب (من المهم دائمًا استشارة طبيب الأعصاب (من المهم بداية الدوار ومسبباته ومدته وتواتره والأعراض المصاحبة له) وفحص عصبي شامل (بما في ذلك اختبار التناسق والرأرأة والمشي). عندها فقط يمكن لطبيب الأعصاب المتمرس تقييم الاختبارات الإضافية التي قد تكون ضرورية. مثل اختبار ديكس-هالبايك أو اختبار AEP أو القدرات السمعية المستحثة أو القدرات العضلية المستثارة الدهليزية أو مخطط السمع (اختبار السمع) أو قياس الطبلة أو تخطيط الرأرأة بالفيديو أو تخطيط الصماخ الكهربائي أو التصوير المقطعي المحوسب أو التصوير بالرنين المغناطيسي
العلاج
يعتمد علاج الدوار على السبب الكامن وراءه. فقط إذا تمكن طبيب الأعصاب من معرفة السبب من خلال الإجراءات المذكورة أعلاه يجب أن يبدأ العلاج. إذا كان السبب مهدداً للحياة مثل السكتة الدماغية الحادة فيجب اتخاذ إجراء فوري. في أغلب الأحيان لا يكون العلاج في هذه الحالة طارئاً. نقدم لك فيما يلي لمحة موجزة عن خيارات العلاج الممكنة. ومع ذلك، فإن أي منها يعتمد على النتائج I التشخيصات.
- مناورات إعادة الوضع لمناورة الارتجاف البطيني الرأسي البطني(مثل مناورة إيبلي أو مناورة سيمونت)
- العلاج الدوائي: مثبطات الدهليز (الميكليزين، البنزوديازيبينات)، الكورتيكوستيرويدات القشرية ومدرات البول، حاصرات بيتا، حاصرات قنوات الكالسيوم، مضادات الاكتئاب، مضادات الاختلاج.
- التمارين البدنية أو العلاج الطبيعي بشكل عام النشاط البدني إيجابي لأن الأذن الداخلية تتدرب على ذلك. يجب تجنب المواقف الخطرة أو خطر السقوط بالطبع.
- نمط الحياة: في حالة الإصابة بالصداع النصفي يجب تجنب حالة الدوار المسبب للصداع النصفي. يمكن العثور على المزيد من علاج الصداع النصفي هنا.
البروفيسور د. ديتليف كومبف - طبيب أعصاب وخبير في الدوار والمشاكل البصرية
البروفيسور كويمبف، أخصائي الدوار والمشاكل البصرية، وهو أستاذ جامعي ألماني أصيل ولد في مدينة سايكينغن بالقرب من فرايبورغ ودرس الطب في هايدلبرغ.
بعد أن أمضى سنة واحدة من الأبحاث في الولايات المتحدة الأمريكية، واصل تعليمه الطبي في مستشفيات جامعة مانهايم وهايدلبرغ ثم انتقل للعمل كنائب رئيس مستشفى الأمراض العصبية في إرلانغن، ومنذ عام 1987 وحتى عام 2010، شغل البروفيسور كومبف منصب مدير مستشفى جامعة الأعصاب في لوبيك بألمانيا حيث عمل كاستشاري أول في طب الأعصاب، وألقى محاضرات ودرّس للطلاب. في عام 2010 انتُخب أميناً عاماً للاتحاد الأوروبي لجمعيات طب الأعصاب (الاتحاد الأوروبي لجمعيات طب الأعصاب) حيث قام بتنظيم مؤتمرات كبيرة في طب الأعصاب والتعليم الإضافي لأطباء الأعصاب في الدول الشرقية مثل روسيا وبيلاروسيا وأوكرانيا ومولدافيا وغيرها.
الهدف من هذه الجهود هو توحيد التشخيص والعلاج العصبي في أوروبا، وفي عام 1998، قام البروفيسور كومبف بتأليف كتاب مهم حول موضوع "طب العيون العصبي السريري" والدوار والمشاكل البصرية الذي نشرته دار نشر ثيمي الشهيرة. كما أنه يتعامل أيضاً مع جميع "أمراض الأعصاب القحفية" التي نشر عنها أيضاً كتاباً في عام 2006، ومنذ أن أنهى مسيرته الجامعية والبروفيسور كومبف يعاين المرضى في عيادته الخاصة في لوبيك ويقضي بعض الأشهر في مايوركا بإسبانيا في مركز الدوار الذي أسسه في مستشفى خوانيدا.
خلال فترة عمله النشط كمدير لمستشفى الأمراض العصبية في جامعة لوبيك، تعامل البروفيسور كومبف مع مجموعة كاملة من الأمراض العصبية بما في ذلك مرض باركنسون والصرع والتصلب المتعدد واضطرابات الدورة الدموية الدماغية والوقاية من السكتة الدماغية واضطرابات الذاكرة والخرف والصداع والصداع والصداع النصفي واعتلال الأعصاب ومتلازمة الساقين المريحة وآلام الظهر وأمراض الأقراص.ولكن قبل كل شيء، ركز على الأنواع العديدة من الدوار (والتي يبلغ عددها حوالي 50 نوعاً) بالإضافة إلى اضطرابات الرؤية أو اضطرابات التوازن. الدوار نفسه هو مجرد مصطلح عام جداً لا يعني أي شيء محدد. يجب التفريق بين الدوار المحدد الذي يعني أن كل شيء يدور وبين الدوار غير المحدد الذي قد يعني فقدان البصر لفترة قصيرة أو الدوار أو اضطراب التوازن، والمشكلة دائماً هي العثور على السبب الكامن وراء ذلك لأنه في كثير من الأحيان قد يكون سبب الأعراض القوية جداً غير مؤذٍ تماماً في حين أن الأعراض الطفيفة قد يكون لها سبب خطير بالفعل. في الحالة الأخيرة، يكون المسار السريع للتشخيص في غاية الأهمية من أجل منع حدوث سكتة دماغية على سبيل المثال. يقع نطاق الدوار بأكمله بين هذين القطبين، وأهم مسألة عند التعامل مع أعراض الدوار هي التاريخ الطبي والتحليل الصحيح للأعراض. في بداية هذا الإجراء سيكون هناك فحص عصبي شامل مع التركيز على حركات العين.
من وقت لآخر سيكون من الضروري إجراء استكشاف نفسي أيضاً لأن الدوار يمكن أن يكون بسبب مشاكل نفسية. يلي ذلك إجراء فحوصات فيزيولوجية عصبية مثل تخطيط كهربية الدماغ أو تخطيط كهربية الدماغ أو تخطيط كهربية الدماغ أو تخطيط كهربية الدماغ أو غيرها وفحص الشرايين القحفية بالموجات فوق الصوتية DUPLEX، والتعاون المشترك مع طبيب الأنف والأذن والحنجرة وطبيب العيون وربما طبيب العظام والمختبر المؤهل. على الرغم من وجوده في دبي منذ فترة وجيزة فقط، أدرك البروفيسور كومبف أن جميع الخدمات التي يحتاجها لعمله المتخصص للغاية متوفرة في دبي، والتي يقدمها في الغالب زملاؤه الألمان مثل طب العيون والأنف والأذن والحنجرة وجراحة العظام وأمراض القلب والمختبر. وهذا ما يجعل التشخيص والعلاج أكثر سهولة لأنهم جميعاً يتبعون نفس المعايير الألمانية العالية ويتيح التواصل غير المعقد بينهم الحصول على نتائج مضمونة. يكرس البروفيسور كومبف بعضاً من وقته في الوقت الحالي للقاء هؤلاء الزملاء والتعرف عليهم من أجل ضمان أفضل النتائج لمرضاه. وكمشاكل رئيسية في هذا المجال، يلاحظ البروفيسور كومبف حتى الآن العلاج الطبي الخاطئ في كثير من الأحيان للمرضى الذين يعانون من مرض باركنسون أو الصرع، وعدم وجود تدابير وقائية للسكتة الدماغية وغيرها من أمراض الأوعية الدموية وكذلك علاج الألم فيما يتعلق بأنواع عديدة من الصداع أو اعتلال الأعصاب الناجم عن مرض السكري. والأهم من ذلك كله هو اهتمامه بالأشخاص الذين يعانون من الدوخة والدوار الذي يعد من أكثر الشكاوى انتشاراً في عيادة الأمراض العصبية ولا يجب الاستهانة بالأسباب الخطيرة المحتملة الكامنة وراءه، وسيواصل البروفيسور كومبف إطلاعنا على موضوع الدوار في هذا الموقع.
يمكننا أيضاً مساعدتك في الحصول على أفضل طبيب نفسي وطبيب نفسي ومعالج نفسي متوفر في دبي، الإمارات العربية المتحدة.
© GNC, German Neuroscience Center Dubai (Neurology, Psychiatry, Psychology, Counseling, Dubai, UAE)
آلام أسفل الظهر \ آلام العمود الفقري
In their anatomical course through the body and the limbs nerves might be damaged in various ways, the cause of damage most often being traumatic. Symptoms of nerve damage may be prickling, numbness and pain but also palsy or disorders of the bladder or the rectum. Lower back pain is one of the most common complaints today. Up to 80% of the US-Population will suffer from back pain at least ones in their lives. Back pain or lumbar pain is the largest cause of work-related absence in the United Kingdom.
Very often nerves are trapped at the spinal cord, the backbone or in their course to the limbs. The reason for this may be some injury, a slipped disk or the trapping of a nerve in a bony or connective tissue canal. A typical example is the carpal tunnel syndrome.
What to do? Prior to surgical decompression therapy, reliable neurological diagnostic methods should be applied to locate the damage exactly. Symptomatic therapy including physiotherapy and special back pain therapy might also be of help.
علاج آلام الظهر في دبي
تُعد آلام الظهر من بين أكثر المشاكل الطبية شيوعاً في المجتمع الحديث وإحدى أكثر الحالات التي يعالجها خبراؤنا شيوعاً. يعاني ما يصل إلى 84% من البالغين من آلام الظهر في وقت ما من حياتهم. يمكن أن تحدث آلام الظهر في جميع الأعمار مع بلوغها ذروتها في سن 40-50 عاماً. آلام الظهر هي أكثر أسباب الإعاقة شيوعاً في جميع أنحاء العالم لدى الأشخاص الذين تقل أعمارهم عن 40 عاماً.
يمكن أن يكون لآلام الظهر العديد من الأسباب المختلفة. ولذلك، وكخطوة أولى، من المهم معرفة السبب الكامن وراءه والتخطيط للعلاج المناسب وفقاً له.
يمكن علاج معظم أسباب آلام الظهر بنتائج جيدة ويمكن تجنب الجراحة. وعلاوة على ذلك، هناك تدابير فعالة للغاية لمنع تكرار آلام الظهر.
أنواع آلام الظهر
آلام الظهر الحادة مقابل آلام الظهر المزمنة: غالبًا ما يكون ألم الظهر الحاد ناتجًا عن إصابة أو حركة خاطئة، ويكون ظهوره مفاجئًا ويستمر لساعات أو أيام فقط. يتميز ألم الظهر المزمن بأنه ألم يستمر لأكثر من 12 أسبوعاً.
موقع الألم: الأكثر شيوعاً هو ألم أسفل أو أسفل الظهر، ولكن يمكن أن يكون الألم في منتصف الظهر أو أعلى الظهر أو الرقبة أيضاً. في ألم الظهر المرتبط بالديسك وعرق النسا، غالباً ما نشاهد ألماً منتشراً أسفل الساقين.
شدة الألم: من ألم خفيف إلى ألم لا يطاق
الأعراض / العلامات
يمكن أن تحدث الأعراض بعد رفع أشياء ثقيلة أو ممارسة تمارين بدنية أخرى. ومع ذلك، يمكن أن تحدث أيضاً دون أي نشاط سابق. للأعصاب الطرفية 3 وظائف: الألم والوظيفة الحسية والحركية. وهذا ما يفسر الأعراض.
- آلام الظهر
- ألم في الظهر أو الأرداف أو الساق (عرق النسا)
- فقدان الإحساس أو التنميل أو الوخز في الجلد
- ضعف عضلات الساقين
- قد يؤدي الألم إلى إجهاد العضلات أو تشنج عضلات الظهر. وبالتالي، تضعف الحركة وتتأثر وضعية الجسم.
- هناك عرض خطير للغاية يسمى انضغاط ذنب الفرس. ويعرّفه أطباء الأعصاب بأنه خدر في الساقين وخلل في المثانة/الأمعاء وعجز جنسي. وهذا يتطلب جراحة عاجلة.
- ألم الرقبة
- ألم في الرقبة والكتف والذراع والصدر والصداع
- دوار، دوار، دوار، دوار، دوار، طنين الأذن، اضطرابات بصرية
- خدر في الذراع واليدين
- ضعف في الذراع واليدين
- قد يؤدي الألم إلى إجهاد العضلات أو تشنج عضلات الظهر. وبالتالي تضعف الحركة وتتأثر وضعية الجسم.
الأسباب
بما أن آلام الظهر يمكن أن تكون ناجمة عن العديد من الحالات المرضية المختلفة، فلا بد من إجراء فحص شامل لمعرفة السبب الحقيقي.
بعض الأسباب الأكثر شيوعًا والحالات الكامنة وراءها هي:
- أمراض الأقراص
- هشاشة العظام، الانزلاق الفقاري، الانزلاق الفقاري، الكسور، هشاشة العظام، تضيق العمود الفقري، خلل في مفاصل أسفل الظهر
- الحوادث وإجهاد العضلات
- السرطان مثل النقائل العظمية وغيرها
- العدوى مثل التهاب العظم والنقي والسل والتهاب القرص والخراج فوق الجافية وغيرها
- الأوعية الدموية مثل تمدد الأوعية الدموية الأبهري البطني والورم الدموي فوق الجافية وغيرها
- أمراض الروماتيزم مثل التهاب المفاصل وغيرها
أسباب أخرى لآلام الظهر
- الألم الذي ينشأ في الأعضاء القريبة من العمود الفقري، مثل المعدة أو الكلى أو المثانة، ويمكن أن ينتشر إلى ظهرك.
- يمكن أن يسبب تورم الشريان الأورطي - وهو الوعاء الدموي الرئيسي الخارج من القلب - ألمًا في الظهر.
- الألم العضلي الليفي العضلي - ألم منتشر على نطاق واسع وإيلام في الجسم - يمكن أن يسبب آلام الظهر.
- يمكن أن تؤذي الأمراض الالتهابية وقرحة المعدة والتهابات المسالك البولية ظهرك.
- النساء: في حالة النساء، يمكن أن تتسبب حالات مثل الحمل والأورام الليفية (أورام الرحم) أو مرض مثل بطانة الرحم المهاجرة في حدوث آلام الظهر.
- الرجال: في حالة الرجال، يمكن أن يكون تمزق الخصية أو التواء الخصية سبباً في ذلك.
يمكن أن يكون هناك العديد من أسباب آلام الظهر، لذلك فإن استشارة أخصائي الرعاية الصحية ضرورية لمعرفة السبب الدقيق.
فيما يلي بعض الأسباب الأكثر شيوعًا بمزيد من التفصيل
داء الفقار
يمكن أن يتسبب التقدم في العمر في إضعاف عضلاتنا وعظامنا وأقراص العمود الفقري تدريجياً. يمر الجميع بعملية ضعف العمود الفقري هذه، ولكن ليس بالضرورة أن يكون ذلك سبباً للألم.
تقع أقراص العمود الفقري بين الفقرات (العظام المكونة للعمود الفقري) وتعمل كممتصات للصدمات. ومع انكماشها مع مرور الوقت، تقل المسافة بين الفقرات وفي الوقت نفسه تبدأ النتوءات العظمية في النمو على طول حواف الفقرات والمفاصل.
في المصطلحات الطبية، يشار إلى هذه الحالة باسم داء الفقار.
وبينما تتقلص الأقراص، فإن الجزء الداخلي من القرص، الذي لا يزال أكثر مرونة، يخترق الجزء الخارجي ويضغط على الجذور العصبية القريبة منه. يُطلق أطباء الأعصاب على ذلك اسم القرص الفقري المتدلي. المواقع الأكثر شيوعاً هي أسفل الظهر، L4-L5 وL5-S1 أو الرقبة، C5-6 وC6-7.
عرق النسا
غالبًا ما يرتبط ألم الظهر بالشعور بالخدر أو الوخز أو الألم في الساقين وهي حالة تسمى عرق النسا.
ينشأ عندما يتضرر العصب الفقري (العصب الوركي) - الذي يمتد أسفل الجزء الخلفي من الساقين - أو ينضغط. وغالباً ما يشعر الأشخاص المصابون بعرق النسا بألم شديد في الساقين أكثر من الظهر أو لا يشعرون بألم في الظهر في كثير من الأحيان.
يمكن أن يؤدي الانزلاق الغضروفي أو انزلاق غضروفي أو نتوء عظمي إلى الضغط على العصب الوركي ويسبب الألم أو الخدر على طول مسار العصب. يمكن أن يسبب هذا الألم في أي مكان من أسفل الظهر إلى القدم أو إصبع القدم.
تضيق العمود الفقري
هناك حالة أخرى مرتبطة بألم الظهر وهي تضيق العمود الفقري الذي يتميز بألم في الساقين أو الذراعين أو الظهر أو الرقبة أو اليدين أو القدمين. يمكن أن يبدأ الألم مرة واحدة ويتلاشى أو قد يزداد سوءاً مع مرور الوقت - اعتماداً على مكان الألم. يمكن أن تكون هذه حالة وراثية أو قد تحدث مع التقدم في العمر.
يحتوي العمود الفقري لدينا على قناة تحتوي على أعصاب الحبل الشوكي، ويمكن أن يؤدي تضييق هذه القناة إلى تضيق القناة إلى تضيق العمود الفقري. يولد بعض الأشخاص بقناة ضيقة وبعضهم قد يعاني من تضيق المساحة في وقت لاحق من حياته. يمكن أن يؤدي ضيق المساحة إلى الضغط على الأعصاب التي تمر عبر هذه القناة، وينتج عن ذلك الشعور بالألم أو الخدر في أجزاء مختلفة.
إلى جانب المناطق الأخرى، يمكن أن تتأثر كلتا الساقين أو إحدى الساقين، ويكون الألم أكثر حدة في الساقين أكثر من الظهر. يشعر بعض الأشخاص بالراحة عندما يجلسون أو يمشون وهم منحني الظهر قليلاً.
عوامل الخطر
- السمنة
- ضعف الصحة البدنية
- سوء التغذية
- التدخين
- الأعمال اليدوية الشاقة
- أسباب نفسية مثل الاكتئاب والمشاكل المتعلقة بالعمل وغيرها.
- الحمل
- الطقس؟ لا! ترتبط آلام أسفل الظهر عادةً بتغيرات الطقس. ولكن يبدو أن هذا غير صحيح.
التشخيص
تعتمد الإجراءات التشخيصية المستخدمة على التاريخ الطبي الكامل للمريض والفحوصات البدنية التي تحدد ما إذا كان هناك أي حالة خطيرة كامنة يمكن أن تكون سبباً للألم. لا يمكن لمقدم الرعاية الصحية تحديد سبب آلام الظهر والعلاج المناسب إلا بعد إجراء فحص شامل للظهر واختبارات عصبية. قد يجري الطبيب عدة اختبارات لتحديد السبب الدقيق لآلام الظهر. تتضمن هذه الفحوصات ما يلي;
- الاستشارة
- الفحص البدني
- الفحص العصبي
- تخطيط كهربية العضل(EMG): يفحص النشاط الكهربائي في أعصاب العمود الفقري. وهي تقنية طفيفة التوغل تساعد في تحديد تلف الأعصاب المسبب لآلام الظهر.
- سرعة التوصيل العصبي (NCV) سرعة التوصيل العصبي (NCV) سرعة التوصيل العصبي (NCV) هو اختبار تشخيصي يقيس سرعة انتقال النبضات الكهربائية عبر الأعصاب في الجسم
- الأشعة السينية: يتم إجراء ذلك لمعرفة ما إذا كان هناك نوع من الخلع أو الكسر أو تنكس العظام.
- التصوير بالرنين المغناطيسي: عادةً ما يتم إجراء فحص التصوير بالرنين المغناطيسي للحصول على نظرة عامة مفصلة لعمودك الفقري. يساعد ذلك في تحديد حتى التغييرات والمشاكل الصغيرة.
- التصوير المقطعي المحوسب: يساعد في الحصول على صورة كاملة ومفصلة لعظامك. يتضمن أشعة سينية متعددة ويساعد في تشخيص آلام الظهر من خلال توفير صورة ثلاثية الأبعاد لعظامك.
متى تزور الطبيب
آلام الظهر شائعة وعادةً ما تتحسن في غضون أيام قليلة، ولكن هناك بعض الحالات التي يجب عليك فيها زيارة الطبيب:
- يزداد ألمك سوءًا يومًا بعد يوم
- إذا استمرت لأكثر من أسبوع أو أسبوعين
- إذا كنت غير قادر على أداء مهامك الروتينية
- لديك ألم شديد يعيقك عن ممارسة أنشطتك
- كنت تواجه مشاكل صحية أخرى مثل الحمى أو صعوبة في انتصاب القضيب
العلاج والوقاية
90% من حالات آلام الظهر الحادة تتعافى تمامًا. لا يزال المرضى الذين يعانون من آلام الظهر والرقبة تحت الحادة أو المزمنة (3 أشهر) لديهم توقعات إيجابية للتشخيص، ولكن ليس بنفس درجة إيجابية آلام الظهر الحادة. علاوة على ذلك، يختلف علاج آلام الظهر أو آلام الرقبة المزمنة عن علاج الآلام الحادة.
يجب ألا يكون هناك علاج بدون فحص مناسب. قبل الخوض في التفاصيل، سنجيب على الأسئلة الأكثر شيوعاً التي يطرحها المرضى:
- هل أحتاج إلى إجراء عملية جراحية؟ أي جراحة هي ضرر محتمل للمريض. لذلك، يجب أن يكون هناك مؤشر واضح. ولحسن الحظ فإن أقل من 2% فقط من المرضى الذين يعانون من آلام الرقبة أو الظهر يحتاجون إلى تدخل جراحي.
- هل أحتاج إلى البقاء في السرير؟ إذا كان الألم حاداً، فستستلقي على الأرجح على أي حال. إذا كانت عضلاتك متشنجة والحركة ضعيفة فليس لديك الكثير من الاحتمالات الأخرى. بعد بدء العلاج لا يوجد تأثير مفيد للراحة في الفراش لفترة طويلة. وعلاوة على ذلك، يمكن أن تحدث مشاكل أخرى مثل الجلطة.
كيفية التعامل مع آلام الظهر
هناك العديد من الأشياء التي يمكنك القيام بها لتخفيف آلام الظهر. يعد البقاء نشيطاً والحفاظ على نمط حياة صحي طريقة جيدة للبدء. الراحة مهمة ولكن منع ظهرك من أي حركة يمكن أن يفاقم الألم ويبطئ عملية الشفاء. غالباً ما تؤدي التمارين الخفيفة إلى تسريع عملية التعافي.
تشير الأبحاث أيضًا إلى أن استجاباتك العاطفية تلعب أيضًا دورًا مهمًا في تسريع عملية التعافي من آلام الظهر. لذا، يجب على المرء أن يتعلم كيفية التعامل مع التحديات العاطفية للتحسن بشكل أسرع. إذا استغرقت آلام ظهرك وقتاً طويلاً حتى تتحسن، يجب عليك زيارة مقدم الرعاية الصحية.
البقاء نشيطاً وممارسة التمارين الرياضية لآلام الظهر
البقاء نشيطاً هو أول شيء يمكنك القيام به لتخفيف آلام ظهرك. فالتمرين أو الحركة المنتظمة تجعل ظهرك مرناً وتحافظ على قوة العضلات الداعمة للعمود الفقري. ويساعد ذلك أيضاً في تقليل الضغط على مفاصلك وعظامك.
قد تشعر بألم في البداية في ظهرك، لكنه لن يسبب أي ضرر. ابدأ بتمرين خفيف وقم بزيادة المدة والشدة تدريجياً. فعدم ممارسة التمارين أو الحركة لفترة طويلة يجعل عضلاتك أضعف وأكثر صلابة، مما يؤدي إلى زيادة ألم الظهر.
تخفف التمارين المنتظمة من آلام الظهر تدريجياً. كما أنها تفرز مواد كيميائية مخففة للألم - المعروفة باسم الإندورفين - والتي لا تساعد فقط في تخفيف الألم بل تحسن المزاج أيضاً.
يمكنك أيضًا تناول مسكنات الألم بتوصية من مقدم الرعاية الصحية الخاص بك قبل القيام بأي تمارين. وبالتدريج ستحصل على ظهر أقوى وأكثر مرونة مما يقلل من الألم.
تمارين لآلام الظهر
هناك الكثير من التمارين التي يمكنك اختيارها للمساعدة في تخفيف آلام الظهر. بعضها
- السباحة: إنها واحدة من أفضل التمارين الخفيفة على ظهرك. هذا التمرين منخفض التأثير لا يضغط كثيراً على مفاصلك ويحسن الدورة الدموية ويخفف من آلام الظهر.
- المشي: إنها طريقة أخرى للحفاظ على نشاطك وتخفيف آلام ظهرك. يمكنك اختيار المدة والوتيرة حسب راحتك وزيادتها تدريجياً.
- اليوغا: تعمل اليوغا بشكل أساسي على تحسين تمدد عضلاتك وتوازنها، وهو ما يمكن أن يكون مفيداً لآلام الظهر.
- البيلاتيس: وهي أيضاً من التمارين الموصى بها لآلام الظهر التي تعمل على تحسين مرونة عضلات الجسم وتعزز قوة وسط الجسم.
- تمارين الصالة الرياضية: يمكن أن تساعد التمارين الرياضية المختلفة التي يتم أداؤها عادةً في صالة الألعاب الرياضية، مثل تمارين القوة وتمارين القلب والأوعية الدموية في تحسين اللياقة البدنية وصحة العمود الفقري بشكل عام.
فقط تذكر أن تتحلى بالصبر وتذكر أن المفتاح هو العثور على التمرين المناسب، ودمجه تدريجياً وأداءه باستمرار.
الأدوية
- تعمل مسكنات الألم الشائعة على تقليل الألم والتورم والالتهاب. وتُستخدم عادةً لعلاج آلام الظهر الحادة. ومع ذلك، وجدت دراسات جديدة أن هذه الأدوية غير كافية في العديد من حالات الألم المزمن، في حين أن مضادات الاكتئاب ومضادات التشنجات يمكن أن يكون لها تأثيرات ملحوظة على العديد من أشكال آلام العظام والمفاصل المزمنة. وعلاوة على ذلك، يجب أن تؤخذ في الاعتبار القدرة الإدمانية للمواد الأفيونية.
- تساعد مرخيات العضلات على التخلص من تشنج العضلات. وبالتالي، يمكن إيقاف الحلقة المفرغة من الألم - تشنج العضلات - ضعف الحركة والوضعية - الألم.
- مضادات الاكتئاب شائعة الاستخدام وفعالة للغاية في علاج آلام أسفل الظهر المزمنة.
- تستخدم مضادات التشنجات (أدوية لمنع النوبات) بنجاح في علاج آلام الظهر المزمنة.
التحفيز الكهربائي للأعصاب عبر الجلد (TENS)
التحفيز الكهربائي للأعصاب عبر الجلد (TENS) هو طريقة معتمدة من إدارة الغذاء والدواء الأمريكية (FDA) وشائعة الاستخدام في علاج الألم الحديث. ويُستخدم في العديد من أشكال الألم الحاد والمزمن.
الوخز بالإبر الصينية
قد يكون الوخز بالإبر الصينية مفيداً كعلاج مساعد لآلام أسفل الظهر.
العلاج الطبيعي، والتدليك، والعلاج الوظيفي
يمكن استخدام العلاج الطبيعي والتدليك والعلاج الوظيفي لتخفيف الألم واستعادة الوظيفة (ولكن لا يتم تشجيع هذا العلاج في المرحلة المبكرة من الإصابة)
العلاج الجراحي
العلاج الجراحي بما في ذلك استئصال الفقرات القطنية المجهرية القطنية، وتثبيت العمود الفقري، واستئصال الصفيحة الفقرية، والعلاج بالمنظار، واستئصال القرص بالمنظار عن طريق الجلد
العلاج السلوكي المعرفي السلوكي (CBT)
لقد تم التقليل من أهمية العلاج السلوكي المعرفي لفترة طويلة، ولكن كما أثبتت الدراسات الجديدة أنها فعالة للغاية. وفي بعض الحالات تكون أكثر فعالية من الأدوية، مع آثار جانبية أقل. وقد أظهرت دراسة حديثة نشرتها الجمعية الأمريكية لعلم النفس أنه عندما يتعلق الأمر بالألم المزمن، فإن التدخلات النفسية غالباً ما توفر راحة أكثر من الأدوية الموصوفة أو الجراحة دون التعرض لخطر الآثار الجانبية، ولكنها تستخدم بشكل أقل بكثير من العلاجات الطبية التقليدية
تعديلات نمط الحياة
إجراء تعديلات على نمط الحياة للقضاء على عوامل الخطر، مثل السمنة وسوء الصحة البدنية وسوء التغذية والتدخين والأعمال اليدوية الشاقة.
مجموعات الدعم هي عبارة عن اجتماعات شهرية تضم من 5 إلى 10 أشخاص، لديهم شيء واحد مشترك، وهو ضعف جودة الحياة بسبب مرض مزمن.
بالنسبة للمشاكل المتعلقة بعلم النفس والطب النفسي، يمكنك دائمًا استشارة طبيب نفسي أو طبيب نفسي أو للاستشارة النفسية فإن معالجينا النفسيين متاحون دائمًا لمساعدتك.
بالنسبة للمشاكل المتعلقة بعلم النفس والطب النفسي، يمكنك دائمًا استشارة طبيب نفسي أو طبيب نفسي أو للاستشارة النفسية فإن معالجينا النفسيين متاحون دائمًا لمساعدتك.
اضطرابات النوم
المرض
اضطراب النوم: علاج الأرق وأعراضه وأسبابه وأكثر من ذلك
هل تعيش في دبي وتعاني من الأرق أو اضطرابات النوم؟ سنوضح لك كيفية الحصول على نوم أفضل. لكن انتبه، إنه عمل حقيقي!
يعاني كل ثلث الأشخاص في دولة الإمارات العربية المتحدة من اضطرابات النوم لمرة واحدة على الأقل. النوم الصحي ضروري لصحتنا البدنية والعقلية. فهو يسمح بتجديد الجسم والتعامل مع الأحداث والانفعالات التي مررنا بها خلال اليوم. ولكن كم من الوقت يحتاج الشخص للنوم؟ في الواقع لا يوجد وقت نوم عام صالح. فلكل كائن حي إيقاع بيولوجي، وبالتالي فإن البعض "ينام مبكرًا" أو "ينام متأخرًا". تختلف الحاجة إلى النوم باختلاف الشخص وعمره وسلوكه في النوم. ومع ذلك، بشكل عام، يحتاج الشخص بشكل عام إلى 7 إلى 8 ساعات من النوم المتواصل ليشعر بالراحة.
التعريف
الأرق / اضطرابات النوم هي واحدة من أكثر الشكاوى شيوعًا في العالم. يعاني أكثر من 60 مليون شخص بالغ من الأرق في الولايات المتحدة الأمريكية فقط. 30٪ إلى 50٪ من السكان يعانون من الأرق أو مشاكل النوم الأخرى. وفي دبي على وجه الخصوص - وهي بيئة عمل عالية الإنتاجية - يعتبر الأرق من الشكاوى الشائعة جداً.
يتسم الأرق/اضطرابات النوم بصعوبة الخلود إلى النوم و/أو الاستمرار في النوم، والاستيقاظ كثيرًا أثناء الليل، والاستيقاظ في وقت مبكر جدًا في الصباح والشعور بالتعب عند الاستيقاظ. وقد يؤثر ذلك سلباً على القدرة على العمل أثناء النهار ويسبب التهيج أو الاكتئاب أو القلق. بالنسبة للمرضى الذين يعانون من اضطرابات النوم، غالباً ما يكون من الصعب الانتباه أو التركيز على المهام أو التذكر. قد يسبب الأرق أيضاً صداع التوتر وبسبب انخفاض الانتباه قد يزيد من الأخطاء والحوادث. قد يكون الأرق اضطراباً مستقلاً أو ثانوياً لحالة طبية.
النماذج
يميز المرء شكلين من الأرق: الأرق الأولي والثانوي. الأرق الأولي هو الأرق الذي لا يرتبط مباشرةً بأي حالة أو مشكلة صحية أخرى، مثل الأسباب الطبية أو النفسية أو البيئية. أما الأرق الثانوي فهو نتيجة لأسباب أخرى مثل المرض (الاكتئاب والربو والتهاب المفاصل والسرطان) والأدوية والقلق المفرط والألم. الاكتئاب هو السبب الرئيسي للأرق الثانوي.
علاوة على ذلك يميز المرء بين الأرق الحاد والمزمن. فهو يختلف من حيث مدة استمراره وعدد مرات حدوثه. يمكن أن يأتي ويذهب وقد تكون هناك أوقات لا يعاني فيها المريض من مشاكل في النوم. يختلف في مدة استمراره وعدد مرات حدوثه. يمكن أن يأتي ويذهب وقد تكون هناك أوقات لا يعاني فيها المريض من مشاكل في النوم.
الأنواع
الأرق: يعاني الشخص من الأرق إذا كان يعاني من صعوبة في الخلود إلى النوم (أرق بداية النوم)؛ إذا كانت نوعية ومدة النوم متقطعة أثناء الليل أو الاستيقاظ المبكر في الصباح ولا يستطيع الشخص العودة إلى النوم (الأرق النهائي).
اضطرابات دورة النوم والاستيقاظ: يحدث عندما تضطرب الساعة الداخلية للشخص للنوم في وقت الظلام والاستيقاظ في وقت الضوء (على سبيل المثال بسبب تغيير المنطقة الزمنية أو العمل بنظام الورديات)
الأرق الطفولي: يتميز بأفعال أو أحداث غير طبيعية تحدث أثناء النوم (مثل المشي أثناء النوم أو الذعر أثناء النوم)
التغفيق: هو اضطراب عصبي يعبر عنه بالنعاس المفرط أثناء النهار.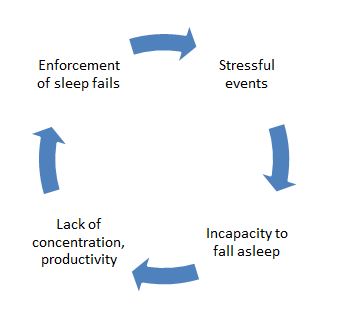
الأسباب
تم ذكر أسباب الأرق الثانوي أعلاه. أسباب الأرق الأولي الحاد يمكن أن تكون شكوى عاطفية أو جسدية أو إجهاد (مهني أو خاص) أو مرض أو عوامل بيئية مثل الضوضاء أو الضوء أو درجات الحرارة الشديدة التي تضعف جودة النوم أو الأدوية أو التدخلات في جدول النوم الطبيعي. أما أسباب الأرق الأولي المزمن فيمكن أن تكون الاكتئاب أو/و القلق، والإجهاد المزمن، والألم أو عدم الراحة أثناء الليل.
في كثير من الأحيان يمكن أن يسبب الشعور بالتوتر الأرق. يمكن للأحداث المجهدة التي حدثت خلال النهار ولم نتمكن من التخلص منها حتى المساء أن تمنعنا من النوم. وتبدأ حلقة مفرغة حيث يرغب الشخص في النوم بشكل أفضل في اليوم التالي ويحاول أن ينام بشكل أفضل في اليوم التالي ويحرص على النوم ولكنه يحقق العكس: قلة النوم.
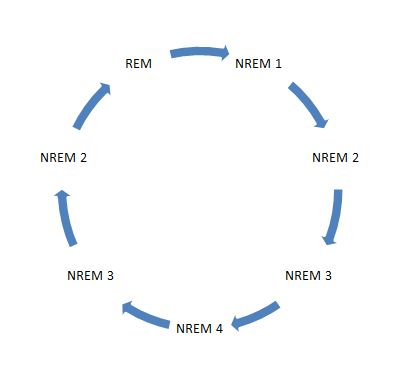
سبب آخر هو نوع النوم. في الواقع، إن عمق النوم وطوله يميزان نوعيته. تميز دورة النوم لدينا مرحلتين رئيسيتين: مرحلة حركة العينين غير السريعة (NREM) التي تتكون من 4 مراحل تنتقل من النوم الخفيف إلى النوم العميق وتستمر لمدة 90 دقيقة. تساعد هذه المرحلة الجسم على التجدد. مرحلة حركة العين السريعة (حركة العين السريعة)، والمعروفة أيضًا باسم نوم الأحلام، والتي تساعد على التعامل مع الأحداث والانفعالات التي مر بها خلال اليوم. لا يشعر الشخص بالراحة حتى لو نام 8 ساعات بسبب انقطاع الدورة: عندما يستيقظ الشخص في لحظة مرحلة النوم العميق في حركة العين غير السريعة (NREM)، يمكن أن يشعر بأنه لم يحصل على قسط جيد من الراحة أثناء الليل. كما يمكن أن يتأثر تجدد الجسم إذا لم يتمكن الشخص من الوصول إلى مرحلة النوم العميق بعد الخلود إلى النوم وبدلاً من ذلك يستيقظ باستمرار. الدورة المثالية للنوم المتجدد موضحة في الرسم البياني أدناه:
وأخيراً يمكن أن تحدث اضطرابات النوم أيضاً بسبب عوامل خارجية مزعجة: إن درجة حرارة الغرفة المنخفضة جدًا، والوسادة المسطحة/المرتفعة جدًا أو الناعمة/القاسية جدًا، والمرتبة القاسية/الناعمة جدًا، واللحاف "قليل التهوية" من عوامل عدم الراحة في النوم. إليك بعض التوصيات: يوصى بتهوية الغرفة قبل الخلود إلى النوم. من المهم اختيار وسادة تسمح بمحاذاة العمود الفقري بشكل مثالي. يجب استخدام مرتبة متوسطة الصلابة لتجنب الضغط على العضلات وتوفير الدعم للظهر والرقبة والساقين. إذا أمكن، اختر ألحفة مصنوعة من مواد طبيعية (الريش والحرير والقطن) لأنها أكثر قابلية للتنفس وتجنب الشخص التعرق والاستيقاظ واضطراب النوم.
التشخيص
تخطيط النوم هو أداة قوية لتشخيص اضطرابات النوم. تخطيط النوم هو تسجيل شامل للتغيرات الفسيولوجية التي تحدث أثناء النوم مثل موجات الدماغ ومستوى الأكسجين في الدم ومعدل ضربات القلب ومعدل التنفس وكذلك حركة العينين والساقين. ويستخدم لتشخيص أو استبعاد العديد من أنواع اضطرابات النوم، بما في ذلك التغفيق وحركات الساقين المضطربة وحركة العينين والساقين وسلوك حركة العين السريعة والباراسومنياس والسهر والأمراض المرتبطة بالصرع والشخير وتوقف التنفس أثناء النوم. ومن ناحية أخرى، قد تتسبب الاضطرابات النفسية المرتبطة بالتوتر أو غيرها من الاضطرابات النفسية في حدوث اضطرابات النوم أو العكس، تماماً مثل الفراش غير المناسب.
لكل هذه الأسباب، من الأهمية بمكان تحليل عادات النوم والنوم بدقة من أجل تحديد التشخيص الصحيح بشكل فردي بمساعدة طبيب الأعصاب وما يتبع ذلك من إمكانيات علاج اضطرابات النوم. لا يمثل الاستخدام الوحيد للعقاقير المنومة حلاً مثالياً بل قد يكون خطيراً لأنه قد يؤدي إلى التبعيات كأثر جانبي غير مرغوب فيه.
كيفية الاستعداد لاختبار اضطرابات النوم
لا توجد تحضيرات كبيرة ضرورية. يُنصح المريض بعدم تناول أي أدوية للنوم أو تناول الكحول أو المشروبات التي تحتوي على الكافيين قبل هذا الاختبار.
عوامل خطر اختبار اضطرابات النوم
تخطيط النوم هو إجراء غير جراحي. لا توجد مخاطر، باستثناء ربما بعض التهيج الجلدي الناجم عن المادة اللاصقة المستخدمة لتثبيت المستشعرات على الجلد. ولذلك فهو إجراء رائع للأطفال أيضاً.
آلية اختبار اضطرابات النوم
يتم وضع أسلاك الاستشعار الفسيولوجية على المريض من أجل تسجيل ما يلي:
- EEG (مخطط كهربية الدماغ)
2. EOG (مخطط كهربية القلب)
3. EMG (مخطط كهربية العضل)
4. ECG (مخطط كهربية القلب)
5. تدفق الهواء (جهاز استشعار الثرمستور أو المزدوجات الحرارية)
6. الجهد التنفسي (مستشعر الجهد البلوري البيزو)
7. تشبع الأكسجين (مقياس التأكسج النبضي)
إجراء اختبار اضطرابات النوم
- في مختبر النوم أو المستشفى
بالنسبة للاختبار القياسي، يأتي المريض - الذي يعاني من اضطرابات النوم - إلى مختبر النوم في وقت مبكر من المساء، وعلى مدار الساعة أو الساعتين التاليتين يتم إدخاله إلى الإعداد و"توصيل الأسلاك" بحيث يمكن تسجيل قنوات متعددة من البيانات عندما يغفو. قد يكون معمل النوم في مستشفى أو في مركز. يجب أن يكون هناك دائماً تقني متخصص في النوم وهو مسؤول عن توصيل الأقطاب الكهربائية بالمريض ومراقبة المريض أثناء الدراسة. يجب أن تشرح للمريض عن الإجراء لإبقاء المريض مسترخياً طوال الليل.
يجب أن يكون مختبر النوم مجهزاً بكاميرات فيديو في غرفة المريض، بحيث يمكن تسجيل المريض أثناء نومه. يسمح ذلك للفني بمراجعة الشريط في أي وقت أثناء الاختبار والتحقق مما إذا كانت الأشكال الموجية ذات المظهر الغريب ناتجة عن استيقاظ فعلي أو فترة استيقاظ أو حركات المريض الطبيعية في السرير.- في المنزل
في الوقت الحاضر، قد يقوم أطباء الأعصاب بإجراء دراسات منزلية لتعزيز راحة المريض وتقليل النفقات، وهو ما يصب في مصلحة أي مريض. يتم إعطاء المريض تعليمات شاملة حول كيفية استخدام أداة الفحص. ثم يستخدم الأداة في المنزل في محيط نومه المعتاد ويعيدها في اليوم التالي. تتكون معظم أدوات الفحص من جهاز قياس تدفق الهواء (الثرمستور) وجهاز مراقبة الأكسجين في الدم (مقياس التأكسج النبضي). وهي صغيرة وسهلة الاستخدام وتنتج رسوماً بيانية ممتازة ونتائج أخرى. في المركز الألماني لعلم الأعصاب يتبع أطباء الأعصاب لدينا هذا المسار الجديد ويزودون المرضى - الذين يعانون من اضطرابات النوم - بأداة يمكنهم تطبيقها بسهولة في المنزل بدلاً من وضع المريض في موقف محرج في العيادة لأنهم يدركون أنه قد يكون من الصعب على المريض إجراء دراسة النوم خارج منزله خاصةً في الدول العربية التي لديها مواقيت صلاة وقواعد مماثلة.
سينام المريض مع جهاز الفحص لمدة ليلة إلى ثلاث ليالٍ، ثم يعيد الجهاز إلى طبيب الأعصاب. سيقوم طبيب الأعصاب باسترداد البيانات من الجهاز ويمكنه وضع افتراضات بناءً على المعلومات المقدمة، على سبيل المثال، قد تشير سلسلة من حالات نقص تشبع الأكسجين في الدم بشكل كبير خلال فترات الليل إلى شكل من أشكال الحدث التنفسي (انقطاع النفس). كحد أدنى، سيراقب الجهاز تشبع الأكسجين.
ملخص اختبار اضطرابات النوم
أثبت تخطيط النوم (PSG) أنه أداة مقنعة لتعزيز فهمنا للنوم واضطرابات النوم. إنه إجراء تشخيصي أساسي لتوضيح أسباب اضطرابات النوم وبالتالي تمكين طبيب الأعصاب من تحديد شكل العلاج المناسب.
من الناحية المثالية، ووفقًا للمبادئ التوجيهية الدولية، يتم إجراء دراسات النوم من قبل أطباء الأعصاب بالتعاون الوثيق مع أخصائي الأنف والأذن والحنجرة في مثل هذه الحالات التي تشير نتائجها الأولية إلى وجود مرض خطير، كما هو متبع في المركز الألماني لعلم الأعصاب GNC.يجب أن يكون تقييم اضطرابات النوم متاحًا بسهولة أكبر لمئات الآلاف من المرضى الذين يعانون من اضطرابات النوم الذين لا يزالون يفتقرون إلى التشخيص والعلاج. ستؤدي قلة النوم أو النوم المضطرب بشكل دائم إلى انخفاض التركيز وضعف الكفاءة الشخصية. ولن يؤثر ذلك بشكل خطير على حياة المرضى الخاصة فحسب، بل سيؤثر أيضًا على قدرتهم على العمل اليومي. قد تؤدي اضطرابات النوم، إذا لم يتم تحليلها وتركها دون علاج، إلى حالات خطيرة، بل ومميتة، وإلى تدهور اجتماعي من خلال، على سبيل المثال، فقدان الشخص لوظيفته. أما اليوم، وبفضل تخطيط النوم المتعدد الأوجه، فلا أحد مضطر إلى تحمل مثل هذه المخاطر، حيث إن أطباء الأعصاب والأطباء النفسيين وعلماء النفس في المركز الألماني لعلم الأعصاب يعرفون العديد من الطرق لعلاج اضطرابات النوم بشكل مناسب بعد تحليلها وتشخيص أسبابها بدقة.
اضطرابات النوم، العلاج
هناك طرق فعالة جداً لعلاج اضطرابات النوم هذه الأيام. بل تكمن المشكلة في أن المرضى يترددون في البحث عن المساعدة المتخصصة. وبالتالي يمكن أن تبدأ حلقة مفرغة حيث يكون المصاب خائفًا بالفعل من الذهاب إلى الفراش. ومن الواضح أنه سيكون من الصعب جداً الخلود إلى النوم. إذا كنت تعاني من اضطرابات النوم، فأنت تعرف ما نتحدث عنه. يستخدم المتخصصون مزيجًا من هذه الخيارات العلاجية المثبتة علميًا لعلاج الأرق: النظافة الصحية للنوم، والتحكم في المنبّهات، وتقنيات الاسترخاء، والعلاج بتقييد النوم، والعلاج السلوكي المعرفي والأدوية.
نود تقديم إحدى هذه التقنيات إلى عتبة بابك أو بالأحرى في غرفة نومك. العلاج بالتحكم في التحفيز. إنه فعال جداً ويستخدم بنجاح منذ أكثر من 30 عاماً. يبدو الأمر سهلاً ولكنه ليس كذلك. النقطة المحورية هي قوة إرادتك للحفاظ على هذه القواعد. إنه عمل فعلي. إذا لم تستطع التحكم فيها بمفردك، فقد يساعدك طبيب نفسي.
قواعد العلاج بالتحكم في المنبهات (بوتزين، 1980)
- لا تنامي إلا عندما تشعرين بالنعاس. ضعي في اعتبارك أن الشعور بالنعاس يختلف عن الشعور بالتعب. من المهم أن تكوني على دراية بهذا الفرق.
- استخدمي السرير للنوم والنشاط الجنسي فقط. لا تنخرط في نشاط غير متوافق مع النوم في السرير مثل تناول الوجبات الخفيفة أو مشاهدة التلفاز أو العمل.
- إذا لم تتمكن من النوم أو الاستيقاظ بعد حوالي 10 دقائق، فاترك السرير واذهب إلى غرفة أخرى. ثم عد إلى السرير وكرر ذلك كلما لزم الأمر حتى تغفو. من المهم عدم مراقبة الساعة أثناء القيام بذلك. فتقديرك الشخصي للوقت هو المهم.
- حافظ على وقت الاستيقاظ الصباحي المنتظم بغض النظر عن مقدار النوم الذي حصلت عليه في الليلة السابقة. سيساعد ذلك على تنظيم الجدول الزمني للساعة البيولوجية (24 ساعة)، وإذا لم تنم جيدًا في إحدى الليالي، فإن الدافع للنوم سيكون أعلى في الليلة التالية.
- تجنب القيلولة. فهذا يمنع تقليل النوم في وقت مبكر من النهار مما يجعل من الصعب الخلود إلى النوم ليلاً.
لماذا ينجح الأمر؟ يطلق عليه علماء النفس اسم التكييف. التكييف هو نوع من التعلم كان له تأثير كبير على المدرسة الفكرية في علم النفس المعروفة باسم السلوكية. التكييف الخاطئ هو مشكلة رئيسية تحدث في الأرق المزمن. إذا كنت تتقلب في سريرك بشكل متكرر لساعات طويلة، سيتعلم جسمك في النهاية أن يربط بين سريرك والإجهاد والاستيقاظ. ونتيجة لذلك، ستجعلك غرفة نومك مستيقظًا بالفعل. تحاول النقاط المذكورة أعلاه معالجة هذه المشكلة وإعادة تعليم جسمك ربط سريرك بالنوم الصحي. ضع في اعتبارك أن الأمر يستغرق وقتًا وجهدًا لإنجاحه. مثل أي شكل آخر من أشكال التعلم. ومع ذلك، إذا لم يكن ذلك كافياً، فقد يكون العلاج المركب هو العلاج المناسب لك. يمكن أن يشمل ذلك نظافة النوم، وتقنيات الاسترخاء، والعلاج بتقييد النوم، والعلاج السلوكي المعرفي والأدوية.
Insomnia? Just popping sleeping pills? Bad idea! You should…
بعض النصائح الإضافية
- تساعد الرياضة وتقنيات الاسترخاء مثل اليوغا في الحصول على نوم صحي. ومن المفيد ممارستها في الهواء الطلق للحصول على هواء نقي. ولكن تجنب ممارسة الرياضة في المساء أو قبل الخلود إلى النوم، لأن ذلك من شأنه أن يحفز الجسم ويؤخر النوم.
- لا تتناول وجبة ثقيلة أو مشروبات منبهة مثل القهوة أو الصودا أو الكحول قبل النوم. يمكن أن يؤدي النيكوتين أيضاً إلى الشعور بالقلق.
- حاولي الاسترخاء والاسترخاء قبل وقت النوم، حاولي الاسترخاء والاسترخاء قبل وقت النوم، أو انقطعي عن اليوم أو استمعي إلى موسيقى هادئة أو اقرئي قراءات خفيفة. إذا لم تتمكن من إيقاف تدفق الأفكار المجهدة، نظف رأسك بكتابة أفكارك/قائمة مهامك/ الخ على ورقة، وضع الملاحظة في درج. فهذا يساعد على "إخراج" أفكارك و"حبسها".
- قبل الذهاب إلى الفراش لا تشاهد أفلام الرسوم المتحركة والأخبار أو تقرأ الكتب المثيرة.
- يجب أن ترتبط غرفة النوم بالهدوء والسكينة. ويوصى بعدم وجود تلفاز في غرفة النوم لأنه من المثيرات المستمرة.
- تقليل العوامل الخارجية المزعجة مثل الضوء أو الضوضاء.
- إذا لم تكن قادراً على النوم تناول المنتجات الغنية بالمغنيسيوم. أفضل وجبة خفيفة هي الحليب الدافئ مع العسل والموز.
- رائحة الزيوت العطرية (اللافندر أو البلسم أو خشب الصندل) تهدئ الجسم وتعزز النعاس.
- إذا استمر الأرق، يوصى باستشارة طبيب نفسي يطبق تقنيات العلاج السلوكي المعرفي. (العلاج المعرفي وتقييد النوم والاسترخاء).
1o. عندما تتسبب عوامل جسدية أو عصبية في حدوث اضطرابات في النوم، فمن الضروري استشارة الطبيب. من المفيد ملء "يوميات النوم" التي تذكر فيها وقت النوم والاستيقاظ، والأنشطة التي قمت بها والطعام الذي تناولته خلال اليوم والأفكار أو المواقف التي تمنعك من النوم. ستوفر هذه المذكرات الدعم لاكتشاف أسباب الاضطراب.
هل تعلم؟
... أننا نقضي ثلث عمرنا في النوم.
... أن جسم الإنسان مبرمج مرتين في اليوم على النعاس: بين منتصف الليل والسابعة صباحًا وبين الواحدة والرابعة مساءً.
... أننا نقضي 20-25% من وقتنا في الحلم أثناء نومنا.
...أن أينشتاين احتاج إلى 10-11 ساعة من النوم وبنجامين فرانكلين 4 ساعات فقط في الليلة الواحدة!المراجع:
1. Collop NA, Anderson WM, Boehlecke B, et al. المبادئ التوجيهية السريرية لاستخدام أجهزة المراقبة المحمولة غير المراقبة في تشخيص انقطاع النفس الانسدادي النومي لدى المرضى البالغين. فريق عمل المراقبة المحمولة التابع للأكاديمية الأمريكية لطب النوم. J Clin Sleep Med. 2007؛ 3:737-747.
2. التواصل الشخصي: مايكل إي غاريسون RSPGT، المشرف على مركز اضطرابات النوم KUMC.
3. ريشتشافن، ألان. كاليس، أنتوني. دليل المصطلحات الموحدة والتقنيات ونظام تسجيل مراحل النوم لدى البشر. خدمة معلومات الدماغ/معهد أبحاث الدماغ. جامعة كاليفورنيا، لوس أنجلوس، كاليفورنيا. 1986.
4. McDonough, James T. Stedman's Concise Medical Dictionary. 2nd edition. Williams and Wilkins Publishers. بالتيمور، دكتوراه في الطب. 1994.
5- Sheldon SH, Spire J-P, Levy HB. طب النوم للأطفال. W.B. Saunders, Co. Philadelphia, PA. 1992.
6. G. Hayak E. Ruther, Insomnie Schalffosigkeit, 1995.© GNC, German Neuroscience Center Dubai (Neurology, Psychiatry, Psychology, Counseling, Dubai, UAE)
- EEG (مخطط كهربية الدماغ)
الخرف وداء الزهايمر
المرض
خرف الزهايمر في دبي
هل تخشى الإصابة بالزهايمر؟ هل تعاني من فقدان الذاكرة؟ هل تعاني من صعوبات في التركيز؟ لا تخف. نسيان الأشياء لا يعني أنك تعاني بالفعل من خرف الزهايمر. ولكن ما هو خرف الزهايمر في الواقع؟
التعريف
خرف الزهايمر هو مرض مزمن يصيب الدماغ ويبدأ ببطء مع أعراض خفيفة. لا يكفي عرض واحد فقط لتبرير التشخيص. نسيان بعض الأشياء في بعض الأحيان لا يجعل من الخرف الزهايمر مرضاً. مع التقدم في العمر، من الطبيعي تماماً أن تصبح ذاكرتك أسوأ. عندما تكون في سن الستين يكون حفظ المعلومات أصعب مما هو عليه في سن الخمسين، ومع بلوغك سن السبعين يكون الأمر أصعب مما هو عليه في سن الستين. وهذا يعني أنك تنسى دائماً أكثر قليلاً مع تقدمك في السن بطريقة طبيعية. الأمر فردي للغاية كم وسرعة استمرار هذه العملية. ويعتمد ذلك على جنسك وحالتك الصحية العامة والبيئة التي تعيش فيها وتعليمك. وقد وجد في الأبحاث العلمية أن الأشخاص ذوي التعليم العالي أو الشهادات الجامعية أو الوظائف المتطورة، والذين يطلق عليهم "العاملون في الدماغ"، يصابون بمرض الزهايمر بشكل أقل وتأخر في الإصابة به من الأشخاص الذين يعملون بشكل أكثر نشاطاً بدنياً. يمتلك دماغنا الكثير من الموارد لتعويض النقص. والدماغ المدرب جيداً يقوم بذلك بشكل أفضل من الدماغ "الكسول".
الأسباب
لا يوجد مرض واحد فقط يسبب الخرف. هناك أنواع مختلفة من أمراض الخرف مثل الزهايمر أو الخرف الوعائي أو خرف أجسام ليوي. كما يمكن أن تكون متلازمات الخرف ناتجة عن أمراض أخرى مثل السكتة الدماغية وباركنسون واستسقاء الرأس وورم الدماغ وغيرها. تقع على عاتق طبيب الأعصاب مهمة معرفة ما إذا كان الشخص يعاني من الخرف وإذا كان الأمر كذلك، فما هو نوعه. أكثر أمراض الخرف شيوعاً هو مرض الزهايمر. ثاني أكثر أشكال الخرف شيوعًا هو الخرف الوعائي أو مزيج من الخرف الزهايمر والخرف الوعائي.
الأعراض
في المراحل المبكرة من مرض الزهايمر لا يعاني مرضى الزهايمر من تراجع الذاكرة فحسب، بل يعانون أيضاً من أعراض أخرى. يبدو الناس مكتئبين لأنهم يدركون مشاكلهم المتزايدة. يشعرون بالتعب والإرهاق ويحاولون تجنب المهام التي تتطلب جهداً فكرياً. بالفعل في المراحل المبكرة من الخرف يغير الناس سلوكهم. فهم يفقدون الاهتمام بالأشياء التي كانت مهمة بالنسبة لهم من قبل، مثل عملهم أو هواياتهم. يتجنب المرضى الذين يعانون من الخرف التواصل الاجتماعي، ويريدون أن يكونوا بمفردهم أو مع أشخاص مقربين جداً مثل أفراد العائلة. يشعر المحيطون بهم أن هناك خطب ما. في البداية يكون الحديث أو القلق قليلاً جداً. هناك دائمًا أعذار لتفسير التغييرات. ثم عندما تصبح الصعوبات أكثر وضوحًا يشعر الناس بعدم الأمان في كيفية التحدث عنها. مرض الزهايمر موصوم بالعار ومن الصعب مواجهة الحقائق لكلا الجانبين. بالنسبة للشخص الذي يعاني نفس الشيء بالنسبة لأفراد الأسرة أو الأصدقاء.
التشخيص
من المهم أن يكون لديك تشخيص واضح إما للتوقف عن القلق أو لاتخاذ الإجراءات اللازمة. ومع ذلك، قد يكون من الصعب التفريق بين النسيان في المراحل المبكرة من العمر ومرحلة مبكرة من مرض الخرف. هناك اختبارات إدراكية خاصة يمكن لطبيب الأعصاب تطبيقها لمعرفة ما إذا كان التغير في الذاكرة لا يزال في مرحلة العمر أم لا. إذا كانت هناك أعراض تغير أكثر من "المسموح به"، فيجب إجراء المزيد من الفحوصات.
يجب استبعاد الأمراض الأخرى مثل الاكتئاب ومتلازمة الإرهاق الناجم عن الإجهاد الزائد والإرهاق الجسدي وغيرها من الأمراض الجسدية. ولكن كيف يمكن معرفة ما إذا كان الشخص يعاني من الخرف؟
أولاً وقبل كل شيء اذهب إلى طبيب الأعصاب وتحدث معه عن مشاكلك. بالفعل من خلال التحدث مع المريض يحصل الطبيب على الانطباع الأول. فهو لا يسمع فقط الشكاوى نفسها. من المهم أيضاً مدة المشاكل وتطورها. الطريقة التي يتحدث بها الشخص، وعلامات اضطرابات الذاكرة في المحادثة، وعلامات فقدان القدرة على الكلام، واضطراب الوقت أو التوجه المحلي، كل هذا قد يظهر بالفعل المضيق الأول لبداية الخرف. يراقب الطبيب أيضًا السلوك العفوي لتكوين رأيه في حالة تكيّفه مع الحالة أم لا. من المهم أيضًا الاستماع إلى أفراد الأسرة أو الأشخاص المقربين الآخرين. فربما يكون لديهم المزيد من المعلومات التي نسيها المريض في النهاية. أو ربما لديهم وجهة نظر أخرى عن التغيرات التي مر بها المريض.
الخطوة التالية هي الاختبارات المعرفية المختلفة. على سبيل المثال اختبار MMSE (اختبار الحالة العقلية المصغر) المستخدم عالمياً، وهو اختبار نفسي لإثبات التوجه، والتراجع، واليقظة، واليقظة، والكلام، والذاكرة وغيرها من الوظائف. ويعطي الفحص العصبي معلومات عن الأنظمة المختلفة للدماغ والأعصاب المحيطية والعضلات. يتم فحص ردود الفعل والكلام والمشي والإحساس بالجهاز الحركي والرؤية والتوازن والأعصاب القحفية. من المهم البحث عما إذا كانت هناك أي علامات يمكن أن تعطي نصيحة لمرض آخر غير الخرف يسبب المشاكل. يتم إجراء اختبارات الدم، ونادراً ما يتم فحص السائل النخاعي (السائل الدماغي الشوكي). السائل الدماغي الشوكي هو السائل الذي يغطي الدماغ والعمود الفقري بالكامل. ويمكن العثور في هذا السائل الدماغي الشوكي على ببتيدات خاصة تشير إلى الإصابة بمرض الزهايمر (ببتيد تاو، ببتيد بيتا).
إن تخطيط كهربية الدماغ (EEG) هو فحص لا يؤلم، ويمكن مقارنته بتخطيط كهربية القلب (ECG) للقلب. وهو يعطي نظرة عامة جيدة على الوظيفة الدماغية الشاملة. يمكن للاختبارات الفيزيولوجية الكهربية الأخرى مثل AEP (إمكانات الاستثارة الصوتية) أو SEP (إمكانات الاستثارة الحسية) أن تعطي المزيد من المعلومات حول وجود آفة في الجهاز العصبي لاستبعاد مرض آخر. كما تعد الفحوصات بالموجات فوق الصوتية لتدفق الدم الدماغي جزءاً من إجراءات التشخيص. يرسل طبيب الأعصاب المريض إلى تصوير الدماغ بالرنين المغناطيسي أو التصوير المقطعي المحوسب. في المراحل المبكرة من الخرف لا توجد علامات محددة للمرض. في المراحل الأكثر تقدماً يمكنك العثور على علامات ضمور في أجزاء خاصة من الدماغ (في المنطقة الزمنية hippocampocampussklerosis). ولكن السبب الأكثر أهمية للتصوير بالأشعة في المراحل المبكرة هو مرة أخرى لاستبعاد الأمراض الأخرى التي يجب علاجها بطريقة مختلفة والتي قد يتم شفاؤها.
العلاج
علاج مرض الزهايمر ممكن. يمكن من خلال الأدوية إبطاء تقدم المرض وتثبيت الذاكرة والتركيز والمهارات الحياتية الأساسية. في مرض ألزهايمر تتحلل الخلايا العصبية ووصلات الخلايا العصبية التي لا يمكن استعادتها. ونتيجة لاضمحلال الخلايا العصبية تتناقص مادة الأسيتيل كولين الناقلة. يعوض نوع خاص من الأدوية، وهو ما يسمى "مثبطات الكولينستريز"، هذا النقص جزئياً. وبهذا تتحسن معالجة المعلومات مرة أخرى. هناك مواد أخرى تؤثر على عملية التمثيل الغذائي الدماغي بطريقة مختلفة والتي قد يكون لها أيضًا تأثيرات مستقرة على الوظائف الإدراكية. يجب علاج الأعراض المتزامنة مثل الاكتئاب واضطرابات النوم والقلق والأرق بأدوية أخرى بجانب أدوية الخرف الخاصة.
مقدمو الرعاية
من المهم جدًا التواصل والتعامل الصحيح مع الشخص المصاب. فالكثير من الصبر والتعاطف، والمحيط الهادئ والمعلومات الجيدة لفهم المرض وسلوك المريض ضرورية للغاية. من الصعب والمرهق للغاية رعاية شخص في مرحلة متقدمة من المرض عندما يحتاج الشخص إلى المساعدة في الأنشطة اليومية والنظافة الشخصية والتغذية ويحتاج إلى مراقبة طوال اليوم. يجب على الأسرة استخدام كل المساعدة وخدمات الخط الأمامي التي يمكنهم الحصول عليها أو حضور مجموعات الدعم.
بخلاف ذلك إذا كنت تعتقد أن المشكلة يمكن حلها عن طريق طبيب نفسي أو أخصائي نفسي، فيمكنك حجز موعد معهم أيضاً.© GNC, German Neuroscience Center Dubai (Neurology, Psychiatry, Psychology, Counseling, Dubai, UAE)
السكتة الدماغية
المرض
السكتة الدماغية، CVA (حادث وعائي دماغي، CVI (إهانة وعائية دماغية)، نوبة دماغية
التعريف
تُعرّف السكتة الدماغية الإقفارية، والمعروفة أيضاً باسم CVA (حادث وعائي دماغي) أو CVI (إعاقة وعائية دماغية) أو نوبة دماغية بأنها انقطاع تدفق الدم داخل أحد الشرايين المغذية للدماغ. وبالتالي تفقد مناطق الدماغ المصابة وظيفتها، وإذا لم يتم علاجها في الوقت المناسب، فإن الخلايا العصبية تموت. واعتماداً على المنطقة المصابة يمكن أن يكون للسكتة الدماغية علامات سريرية مختلفة.
الأسباب وعوامل الخطر
الأسباب الأكثر شيوعًا للسكتة الدماغية الإقفارية أو السكتة الدماغية الوعائية هي تصلب الشرايين والانسداد القلبي بعد الرجفان الأذيني. أما الأسباب الأخرى فهي التهاب الأوعية الدموية أو تسلخ الشرايين أو الأمراض التي تسبب فرط التخثر (تخثر الدم). هناك بعض عوامل الخطورة المرتبطة بالسكتة الدماغية الإقفارية أو السكتة القلبية الوعائية الدماغية (CVA): العمر فوق 60 عاماً، جنس الذكور، ارتفاع ضغط الدم، الرجفان الأذيني، داء السكري، عسر شحميات الدم، تدخين السجائر، الصداع النصفي.
الأعراض
تعتمد أعراض السكتة الدماغية الإقفارية أو السكتة الدماغية الوعائية الدماغية على المنطقة المصابة من الدماغ. غالباً ما تحدث الأعراض فجأة وتؤثر على جانب واحد. قد تكون فقدان مفاجئ للرؤية، أو ضعف أحد الأطراف (شلل جزئي)، أو خدر أو فقدان الحواس، أو مشاكل في الكلام أو البلع، أو فقدان الوعي، أو صداع، أو غثيان وغيرها. إذا تعافت الأعراض بالكامل، فإن طبيب الأعصاب يتحدث عن نوبة إقفارية عابرة TIA، وهي نوبة إقفارية عابرة.

التشخيص
السكتة الدماغية الإقفارية أو CVA (حادث وعائي دماغي) هو تشخيص سريري. ومع ذلك، يجب إجراء الاختبارات التالية. التصوير المقطعي المحوسب أو التصوير المقطعي المحوسب للأوعية الدموية، التصوير بالرنين المغناطيسي، تخطيط كهربية القلب (تخطيط كهربية القلب)، تخطيط صدى القلب، فحوصات الدم.
العلاج
العلاج الأكثر فاعلية هو الوقاية من السكتة الدماغية الإقفارية أو السكتة الدماغية الوعائية (حادث وعائي دماغي). وهذا يعني تقليل عوامل الخطر. لتقييم خطر الإصابة بتضيق الشريان السباتي يمكن لطبيب الأعصاب إجراء تخطيط صدى الشريان السباتي خارج الجمجمة (تخطيط صدى الشريان السباتي المزدوج خارج الجمجمة) وتخطيط صدى الشريان السباتي المزدوج عبر الجمجمة. اعتماداً على النتائج يمكن أن يستفيد المرضى من العلاج التدخلي، مثل استئصال باطنة الشريان السباتي. يجب مراقبة ارتفاع ضغط الدم والرجفان الأذيني وداء السكري وعسر شحميات الدم عن كثب ومعالجتها بشكل صحيح. علاوة على ذلك، يجب أن تشمل التغييرات في نمط الحياة: النظام الغذائي والرياضة والحد من التدخين.
في حالة حدوث سكتة دماغية أو سكتة قلبية وعائية (حادث وعائي دماغي)، فإن الوقت هو العامل الأهم. يجب إدخال المرضى وعلاجهم في المستشفى في غضون 3 ساعات. خط العلاج الأول هو انحلال الخثرة الوريدي مع أدوية أخرى.
بعد حدوث السكتة الدماغية أو السكتة القلبية الوعائية الدماغية، يجب على المرضى تناول دواء لمنع حدوث سكتة دماغية ثانية. يمنع هذا الدواء تخثر الدم من التجلط. علاوة على ذلك، فإن إعادة التأهيل المبكر هو ما يحدد التعافي. يجب أن تكون إعادة التأهيل شاملة وتشمل العلاج الطبيعي وعلاج النطق والعلاج المهني والنفسي.
بخلاف ذلك إذا كنت تعتقد أن مشكلتك يمكن حلها بواسطة طبيب نفسي أو أخصائي نفسي، يمكنك حجز موعد معهم أيضاً.
© GNC, German Neuroscience Center Dubai (Neurology, Psychiatry, Psychology, Counseling, Dubai, UAE)
شلل بيل
أسباب مرض شلل الوجه النصفي وعلاجه وأعراضه والتعافي منه والمزيد
شلل بيل هو شلل أو ضعف حاد في عضلات أحد جانبي الوجه. وهو اضطراب عصبي محيطي شائع نسبياً ويمكن أن يصيب الأشخاص من جميع الأعمار، ولكنه أكثر شيوعاً بين 15-45 عاماً.
وقد عانى العديد من المشاهير مثل أنجلينا جولي وأنوبام خير وجورج كلوني وبيرس بروسنان من شلل بيل.
وفي ظل العلاج المناسب، يتعافى معظم المرضى بشكل جيد، على الرغم من أن بعضهم يعاني من ضعف متبقٍالعلامات والأعراض
يسبب شلل الوجه النصفي شللًا حادًا في جميع عضلات الوجه التي يغذيها العصب القحفي السابع (العصب الوجهي). ويكون دائماً أحادي الجانب (جانب واحد) ويشمل عضلات الوجه العلوية والسفلية. قد يعاني الأشخاص في البداية من خدر خفيف في الوجه أيضاً. قد تشمل الأعراض الأخرى ما يلي:
قراءة المزيد
الأسباب
شلل بيل هو، بحكم تعريفه، مجهول السبب، أي بدون سبب محدد. ومع ذلك، يبدو أنه مرتبط بعدوى فيروسية معينة. يمكن العثور على فيروس الهربس (HSV-1) في 80% من المرضى. تشمل العدوى الفيروسية الأخرى فيروس الهربس النطاقي وفيروس النكاف وفيروس الحصبة الألمانية وفيروس نقص المناعة البشرية. كما يجب أخذ داء لايم بعين الاعتبار أيضاً.

التشخيص
بالنسبة لطبيب الأعصاب المتمرس، يعتبر شلل الوجه النصفي تشخيصاً سريرياً في الأساس. في حال الاشتباه في وجود عدوى فيروسية، يمكن النظر في إجراء اختبارات الدم. إذا تعذر استبعاد الشلل المركزي، فقد يتم النظر في إجراء تصوير بالرنين المغناطيسي. للتحقق من التشخيص وللتنبؤ بالنتيجة عادةً ما يتم إجراء فحص سرعة توصيل العصب (NCV).
قراءة المزيد
العلاج
عادةً ما يكون علاج شلل الوجه النصفي فعالاً للغاية ويحقق الأشخاص نتائج جيدة. ومع ذلك، يمكن أن تتفاقم الأعراض خلال الأيام الأولى من العلاج. يجب أن يكون المرضى على دراية بذلك. تكون نتيجة العلاج أفضل إذا بدأ العلاج مبكراً. قد يشمل العلاج ما يلي:
قراءة المزيد
التشخيص
عادة ما تكون نتيجة شلل الوجه النصفي جيدة ويتعافى معظم الأشخاص في غضون أسابيع قليلة. ولكن في 8% من الحالات يكون الشلل متكررًا.
- التشخيص الجيد: شلل جزئي
- سوء التشخيص الشلل التام، وفقدان حاسة التذوق بعد ذلك، وعلم الأمراض في اختبار NCV (سرعة توصيل العصب)
المضاعفات
المضاعفات الأكثر شيوعاً لمرض شلل الأجراس هي مشاكل إعادة التعافي. إذا كان العصب يتعافى وينمو، فقد يتصل عن طريق الصدفة بأعصاب أخرى مما يؤدي إلى حدوث خلل. قد يشمل ذلك:
- دموع التماسيح (البكاء أثناء الأكل)
- التعرق الذوقي (التعرق أثناء الأكل)
- الارتباط بعضلات المضغ (ارتعاش الوجه أثناء الأكل)
فريق الخبراء لدينا
منذ أكثر من عشر سنوات تعتبر GNC العيادة الرائدة في مجال طب الأعصاب في الإمارات العربية المتحدة. جميع خبراء شلل الوجه النصفي لدينا حاصلون على شهادة البورد الألماني ولديهم خبرة مهنية لا تقل عن 25 عاماً. إذا كنت تبحث عن أكثر خبراء شلل الوجه النصفي الموثوقين، فأنت في المكان الصحيح.
يمكننا أيضاً مساعدتك في الحصول على أفضل الأخصائيين النفسيين والأطباء النفسيين والمعالجين النفسيين المتاحين في دبي، الإمارات العربية المتحدة.Testimonials
``It was a great visit thanks! It really helped me.``
``Great service``
``God bless you guys wish you more of success``
``I'm impressed by the Professor and team professionalism``
``Being able to have blood tests and EEG done at the clinic itself was very helpful and convenient. This also allowed my doctor to have fast access to the test results.``
``I am thankful for the service.``
``Excellent doctor``
``The doctor is the best and everyone's very helpful``
As Seen On


الصرع ، النوبات ، التشنجات
الصرع، التشنجات، التشنجات، النوبات، النوبات
الصرع أو التشنجات أو التشنجات أو النوبات الصرعية أو النوبات هي من أكثر الاضطرابات العصبية شيوعاً، حيث تبلغ نسبة الإصابة السنوية من 35 إلى 52 حالة لكل 100 ألف شخص. وهو عبارة عن اضطراب في الجهاز العصبي المركزي يؤثر على نشاط الخلايا العصبية في الدماغ ويتميز بوجود نوبات صرع متكررة وغير مبررة.
لدى المريض نزعة لإظهار نوبات متكررة من أعراض السلوك المضطرب والأحاسيس المضطربة، بما في ذلك فقدان الوعي. يمكن أن يكون للنوبات أو التشنجات عواقب جسدية ونفسية اجتماعية عميقة. ومع ذلك، لا تشير نوبة أو نوبة واحدة إلى الإصابة بالصرع.
لا يمكن تشخيص المرض إلا إذا كان هناك ميل كامن نحو نوبات أو نوبات صرع متكررة وغير مبررة.
الأسباب
لا يوجد سبب محدد للصرع لدى حوالي نصف المصابين بهذه الحالة. يتحدث الأخصائيون عن الصرع العرضي إذا حددوا سبباً مثل ورم في الدماغ. تشمل الأسباب الأكثر شيوعًا للصرع ما يلي:
قراءة المزيد
العلامات والأعراض
يفرق الأخصائيون بين النوبات البؤرية أو المعممة، بناءً على كيفية بدء النشاط غير الطبيعي في الدماغ. تتميز النوبة الصرعية البؤرية بنشاط غير طبيعي في منطقة واحدة فقط من الدماغ ويمكن أن تشمل فقدان الوعي. أما النوبات المعممة فهي...
قراءة المزيد
التصنيف
يُصنف الصرع أو النوبات على أنه(ILAE):
قراءة المزيد
التشخيص
تشخيص الصرع هو عملية من ثلاث خطوات تشمل التحديد السريري للنوبة المحتملة والنظر في التشخيصات التفاضلية وتصنيف النوبة. سيقوم طبيب الأعصاب ب...
قراءة المزيد
العلاج
يمكن لمعظم الأشخاص المصابين بالصرع أن يصبحوا خالين من النوبات أو النوبات عن طريق تناول دواء واحد مضاد للنوبات يسمى الدواء المضاد للصرع.
ينطوي علاج الصرع على...
قراءة المزيد
فريق الخبراء لدينا
منذ أكثر من عشر سنوات تعتبر GNC العيادة الرائدة في مجال طب الأعصاب في الإمارات العربية المتحدة. جميع خبراء الصرع لدينا حاصلون على شهادة البورد الألماني ولديهم خبرة مهنية لا تقل عن 25 عاماً. إذا كنت تبحث عن أكثر خبراء الصرع الموثوق بهم، فأنت في المكان الصحيح.
يمكننا أيضًا مساعدتك في الحصول على أفضل الأطباء النفسيين والأطباء النفسيين والمعالجين النفسيين المتاحين في دبي، الإمارات العربية المتحدة.الوخز والتنميل والضعف والألم والوخز والخدر والضعف والألم
هل تعاني من وخز أو خدر أو ضعف أو ألم وتريد أن تعرف سبب ذلك؟ سيوضح لك هذا الدليل السريع كيفية القيام بذلك.
علاج الوخز والضعف في اليدين والقدمين والساقين: الأعراض والمزيد
المرض هو السبب الكامن وراء المرض (مثل التصلب المتعدد)، والعرض هو كيفية ظهور المرض نفسه (مثل التنميل في الأطراف)
الوخز والخدر والضعف والألم هي الأعراض الأكثر شيوعاً في طب الأعصاب. لماذا؟ علم الأعصاب هو علم الأعصاب (الخلايا العصبية). هناك أنواع مختلفة من الأعصاب في جسم الإنسان:

الخلايا العصبية الحسية (أو الوريدية): إرسال المعلومات من المستقبلات الحسية إلى الدماغ. وللمستقبلات مواقع ووظائف مختلفة:
- العين - الرؤية
- الأنف - الرائحة
- اللسان - التذوق
- الجلد، الأعضاء الداخلية - الإحساس، الاهتزاز، الضغط، الألم
الخلايا العصبية الحركية (أو الوافدة): ترسل المعلومات من الدماغ إلى العضلات أو الغدد.
- العضلات (الأطراف والقلب والأوعية الدموية وغيرها)
- الحشفة (اللعاب وما إلى ذلك)
يتحكم الجهاز العصبي في جميع وظائف جسم الإنسان. ويؤدي تلف العصب إلى فقدان وظيفة معينة
- خدر: تلف العصب الحسي الذي يرسل المعلومات الحسية من الجلد إلى الدماغ
- الوخز: تلف العصب الحسي الذي يرسل المعلومات الحسية من الجلد إلى الدماغ
- الألم: تلف العصب الحسي الذي يرسل المعلومات الحسية من الجلد إلى الدماغ.
- ضعف العضلات: تلف العصب الحركي الذي يرسل نبضات الحركة من الدماغ إلى العضلات
حسناً، الوخز والخدر والضعف والألم هي الأعراض الأكثر شيوعاً في علم الأعصاب وهي ناتجة عن تلف الأعصاب. هذا جيد حتى الآن. الآن يصبح الأمر أكثر تعقيداً بعض الشيء لأننا نريد أن نعرف أين وأي عصب تالف بالضبط. في الأساس هناك موقعان مختلفان محتملان. الجهاز العصبي المركزي (الجهاز العصبي المركزي - الدماغ والعمود الفقري) والجهاز العصبي المحيطي (الجهاز العصبي المحيطي - أعصاب الأطراف والأعضاء الداخلية). الأمر مربك بعض الشيء لأن
يمكن أن يؤدي كلا الموضعين إلى نفس الأعراض التي قد تواجهها.
على سبيل المثال العمى. يعاني المريض من فقدان البصر. يمكن أن يحدث هذا بسبب تلف في المستقبلات العصبية في العين، أو الخلايا العصبية المؤدية من العين إلى الدماغ أو الخلايا العصبية في الدماغ نفسه. يمكن أن يحدث الوخز أو التنميل أو الألم بسبب تلف المستقبلات العصبية في الجلد أو الخلايا العصبية المؤدية من الجلد إلى الدماغ أو الخلايا العصبية في الدماغ نفسه.
والآن يزداد الأمر تعقيداً لأننا نريد معرفة سبب تلف الأعصاب.
يمكن أن يحدث العرض نفسه بسبب العديد من الأمراض المختلفة.
يمكن أن يحدث التنميل بسبب عصب مضغوط أو اعتلال الأعصاب أو التصلب المتعدد أو ورم في الدماغ وما إلى ذلك. وهذا يوضح سبب أهمية معرفة السبب الدقيق لتلف العصب.
الأسباب
- التصلب المتعدد
- السكتة الدماغية، النوبة الإقفارية العابرة (TIA)
- الصداع النصفي
- النوبات
- تلف الأعصاب (الاعتلال العصبي) بسبب داء السكري
- إصابة العصب (مثل إصابة الرقبة وإصابة الظهر)
- الانزلاق الغضروفي في العمود الفقري
- الضغط على أعصابك (يمكن أن يكون بسبب نسيج متندب أو تضخم الأوعية الدموية أو العدوى أو الأورام أو متلازمة النفق الرسغي (الضغط على - عصب في الرسغ)
- الجلوس أو الوقوف في الوضعية نفسها لفترة طويلة
- التهاب النخاع المستعرض (التهاب الحبل الشوكي)
- التهاب الدماغ (التهاب الدماغ)
- مستويات الكهارل غير الطبيعية
- نقص فيتامين B12 أو فيتامين B12 أو فيتامين آخر
- آخرون
سيكون العلاج مختلفًا تمامًا حسب السبب.
باختصار، نحن نعلم أن الوخز والخدر والضعف والألم هي الأعراض الأكثر شيوعاً في علم الأعصاب وهي ناتجة عن تلف الأعصاب. يمكن أن تكون الأضرار في مواقع مختلفة وقد تكون ناجمة عن أمراض كامنة مختلفة.
كيف يمكن لطبيب الأعصاب معرفة سبب الوخز والتنميل والضعف والألم الذي أشعر به؟
سيسألك في الاستشارة عن الأعراض التي تعاني منها. بداية الأعراض، ومستوى الألم، والتغيرات أثناء النهار أو الليل، وتطورها، وموقعها إلخ... في الفحص العصبي سيقوم بفحص الأعراض والتحقق مما إذا كانت على كلا الجانبين، أو تقتصر على منطقة جلدية، أو ردود الفعل، إلخ. علاوة على ذلك بالنسبة للأضرار المحددة هناك فحوصات عصبية محددة مثل NCV (سرعة توصيل العصب)، والقدرات المستحثة، والتصوير بالرنين المغناطيسي إلخ. تتطلب بعض الأمراض مثل التصلب المتعدد فحوصات أكثر شمولاً.
نأمل أن تعطيك هذه المقالة لمحة موجزة وغير طبية للغاية عن عملية التشخيص في حال كنت تعاني من الأعراض العصبية الأكثر شيوعاً من الوخز أو التنميل أو الضعف أو الألم. في حال كان لديك المزيد من الأسئلة، فإن فريقنا يتكون أيضاً من أطباء ذوي خبرة في علم النفس والطب النفسي والعلاج النفسي. من فضلك لا تتردد في الاتصال بنا.
متلازمة النفق الرسغي
You've been plagued by numbness and tingling in your fingers and wrist. You are waking up at night with a "pins and needles" sensation in one hand? There might be other explanations, but the symptoms suggest you may have carpal tunnel syndrome. Is it dangerous? No. But to ignore the symptoms may cause damage of the nerve and the muscles. What is to do?In carpal tunnel syndrome (CTS), one of the nerves to the hand (the median nerve) becomes compressed as it passes through the wrist. There are different causes which can lead to CTS like occupational overstressing of the hands, injuries at the wrist with malposition of the carpal bones, arthritis, pregnancy, diabetes, overweight and others. Also a genetic predisposition is discussed. In many cases, no single cause can be identified. It may be that a combination of risk factors contributes to the development of the condition.
Carpal Tunnel Syndrome Symptoms
The typical symptoms are numbness or tingling in the thumb, index, middle and ring finger, later pricking and painful paraesthesias. Sometimes the whole arm up to the shoulder is affected. This happens during the night or after awaking in the morning; but also with certain hand positions like keyboard typing, holding a phone or reading a newspaper, cycling or motor biking. The symptoms are intensified by overloading the hands by repetitive manual work. At the beginning the discomfort can be reduced by “shaking” the hands. Later a persistent numbness may occur. Left untreated, carpal tunnel syndrome can lead to constant pain and to permanent nerve and muscle damage that could severely limit your ability to use your hands.
Carpal Tunnel Syndrome Diagnostics
If you have persistent signs and symptoms, especially if they interfere with your normal activities and sleep patterns, you should see your neurologist.
Your doctor will conduct a neurological examination. Tests with pressure on the median nerve at the wrist, produced by bending the wrist (Phalen`s maneuver) or tapping on the nerve (Tinel`s sign) can bring on the symptoms in many people. Important is to prove the feeling in your fingers and the strength of the muscles in your hand. Nerve conduction studies (an electrodiagnostic test) can pinpoint damage to the median nerve by measuring how fast electrical impulses move through it. Up to 10 percent of people with carpal tunnel syndrome, however, test is normal when this method is used. Other examinations like electromyogramm, SEPs (sensory evoked potentials), ultra sonic or MRI might be necessary to rule out other conditions like nerve root irritation or compression at the cervical spine.
Carpal Tunnel Syndrome Treatment
Fortunately, for most people who develop carpal tunnel syndrome, proper treatment usually can relieve the tingling and numbness and restore wrist and hand function, especially if you catch the condition early.
Nonsurgical therapy is possible if you have mild to moderate symptoms and the neurological examinations do not show an extensive damage at the median nerve. Medication with anti-inflammatory drugs (NSAIDs) such as Ibuprofen may help relieve pain from carpal tunnel syndrome only in the short term.

- wrist splint
The most effective conservative treatment is nocturnal splinting with a specially wrist splint. If you use it, avoid wearing it all day, since that can weaken your muscles in your wrists and hands. Wearing it all night, however, is recommended. This should be done at least for 3 month.
If the symptoms persist or the nerve conduction velocity becomes worse, surgery has to be considered. Two main types of surgery are used to relieve the pressure on the nerves inside the carpal tunnel: open carpal tunnel release and the newer endoscopic carpal tunnel release. Both are outpatient procedures performed under local anesthesia (the surgeon cuts the ligament along the middle of the palm and inner wrist). Most people make a full recovery, but in some cases (fewer than 5 percent) carpal tunnel syndrome recurs after surgery. This happens more commonly following the endoscopic procedure, which often doesn't open up the tunnel as fully as open release.
متلازمة النفق الرسغي
هل تعاني من ألم وتنميل ووخز في أصابعك ومعصمك؟ هل تستيقظ ليلاً وأنت تشعر بإحساس "الدبابيس والإبر" في إحدى يديك؟ قد تكون هناك تفسيرات أخرى، لكن الأعراض تشير إلى احتمال إصابتك بمتلازمة النفق الرسغي.
ما هي متلازمة النفق الرسغي؟
متلازمة النفق الرسغي (CTS) هي حالة تحدث عندما يتم الضغط على العصب المتوسط وتسبب الإحساس بالألم أو التنميل أو الوخز أو الضعف في اليد. يمتد العصب الناصف بطول الذراع ويمر عبر ممر ضيق في الرسغ يُعرف باسم النفق الرسغي. إذا انضغط العصب في هذا الممر، فقد يتضرر العصب وتحدث الأعراض. العصب الناصف مسؤول عن التحكم في حركة الإبهام والأصابع، باستثناء الإصبع الصغير. وعلاوة على ذلك، فإنه ينقل المعلومات الحسية من اليد والأصابع إلى الدماغ.
الأسباب الشائعة لمتلازمة النفق الرسغي (متلازمة النفق الرسغي)
هناك أسباب مختلفة يمكن أن تؤدي إلى الإصابة بمتلازمة متلازمة الأمعاء المقطعية مثل الإجهاد المهني الزائد لليدين، والإصابات في الرسغ مع سوء وضع عظام الرسغ، والتهاب المفاصل، والحمل، والسكري، وزيادة الوزن وغيرها. كما تتم مناقشة الاستعداد الوراثي. في العديد من الحالات، لا يمكن تحديد سبب واحد. قد تساهم مجموعة من عوامل الخطر في تطور الحالة. تشمل الأسباب الأخرى ما يلي:
- قصور الغدة الدرقية
- السمنة
- التهاب المفاصل الروماتويدي
- الحركات المتكررة مثل الكتابة على الآلة الكاتبة
- داء السكري
أعراض متلازمة النفق الرسغي
تتمثل الأعراض النموذجية في خدر أو وخز في الإبهام والسبابة والوسطى والبنصر، ثم وخز في وقت لاحق وشبه وخز مؤلم. في بعض الأحيان يتأثر الذراع بالكامل حتى الكتف.
وتشتد الأعراض عن طريق التحميل الزائد على اليدين عن طريق العمل اليدوي المتكرر. في البداية يمكن تقليل الانزعاج عن طريق "هز" اليدين. في وقت لاحق قد يحدث خدر مستمر. إذا تُركت متلازمة النفق الرسغي دون علاج، يمكن أن تؤدي متلازمة النفق الرسغي إلى ألم مستمر وإلى تلف دائم في الأعصاب والعضلات قد يحد بشدة من قدرتك على استخدام يديك.
عند إصابتك بمتلازمة متلازمة الأمعاء المقطوعة في مراحلها المبكرة، قد تلاحظ شعورك بالخدر في يديك بالإضافة إلى الإحساس بالوخز. ويحدث ذلك أثناء الليل أو بعد الاستيقاظ في الصباح، وكذلك مع بعض وضعيات اليدين مثل الكتابة على لوحة المفاتيح أو الإمساك بالهاتف أو قراءة الجرائد أو ركوب الدراجات الهوائية أو ركوب الدراجات النارية.
قد تتفاقم الأعراض عند حمل أشياء ثقيلة أو ثني المعصم. وقد ذكر الكثيرون أن هز اليدين قد يخفف من الأعراض، لكن هذا لا يؤدي دائماً إلى زوال الخدر تماماً.
عندما تبدأ أعراض الإصابة بمتلازمة موت العضلات المزمن في التفاقم، قد تجد نفسك غير قادر على الإمساك بقوة عند الإمساك بالأشياء حيث تبدأ عضلات يدك في التقلص. قد تشعر أيضاً بتقلصات عضلية وألم في العضلات. تشمل الأعراض الشائعة الأخرى لمرض متلازمة موت العضلات المزمن ما يلي:
- ألم أو وخز أو وخز أو تنميل في أصابعك و/أو يدك أو كليهما
- الأيدي الضعيفة
- إحساس شبيه بالصدمة في أصابعك
- الإحساس بالحرق أو الحكة في راحة يدك أو إبهامك أو السبابة والوسطى
- في بعض الأحيان يتأثر الذراع بأكمله حتى الكتف
عوامل الخطر
هناك العديد من العوامل المرتبطة بمتلازمة النفق الرسغي على مر السنين. قد لا تتسبب هذه العوامل في الإصابة بمتلازمة النفق الرسغي بشكل مباشر، ولكنها تزيد من خطر تلف العصب المتوسط. تشمل عوامل الخطر ما يلي:
- كسور المعصم أو خلع المعصم
- التهاب المفاصل الذي يشوه العظام الصغيرة في المعصم
- الجنس؛ يشيع الإصابة بمتلازمة الأمعاء المقطعية لدى النساء لأن منطقة النفق الرسغي أصغر لدى النساء مقارنة بالرجال
- الأمراض المزمنة مثل داء السكري
- الحالات الالتهابية مثل التهاب المفاصل الروماتويدي
- الأدوية
- السمنة
- الحمل
- اضطرابات الغدة الدرقية أو الفشل الكلوي
- ظروف مكان العمل التي تتطلب حركة المعصم لفترات طويلة ومتكررة، مثل الكتابة على الآلة الكاتبة
التشخيص
عندما تتطور أعراض الإصابة بمتلازمة الألم الرضحي المزمن وتبدأ في أن تصبح غير محتملة، يوصى بزيارة الطبيب. قد يجري الطبيب فحوصات مثل:
- مخطط كهربية العضلات، حيث يقوم الأطباء بوضع قطب كهربائي رفيع في عضلاتك لقياس نشاطها الكهربائي
- دراسات التوصيل العصبي لقياس الإشارات في أعصاب الذراع واليد
- الموجات فوق الصوتية لفحص الأنسجة والعظام
العلاج والوقاية
يعتمد علاج متلازمة النفق الرسغي على شدة الأعراض التي تعاني منها. قد يوصي الأطباء بما يلي:
- قم بإجراء تغييرات على حياتك اليومية لتجنب حركات المعصم المتكررة والمجهدة
- ممارسة التمارين الرياضية وتمارين الإطالة بشكل متكرر لمساعدة الأعصاب والعضلات على الحركة بشكل أفضل بشكل يومي
- ارتدِ جبيرة إذا نصحك طبيبك بارتداء جبيرة لمنع معصمك من الحركة كثيرًا
- تناول الأدوية المضادة للالتهابات أو حقن الستيرويد للمساعدة في تقليل التورم والالتهاب
- إذا لم ينجح العلاج، فقد يُنصح بإجراء عملية جراحية لزيادة حجم النفق الرسغي وتخفيف الضغط على العصب المتوسط.
لحسن الحظ، بالنسبة لمعظم الأشخاص الذين يصابون بمتلازمة النفق الرسغي، عادةً ما يمكن للعلاج المناسب أن يخفف من الوخز والخدر واستعادة وظيفة المعصم واليد، خاصةً إذا اكتشفت الحالة مبكرًا. يشمل العلاج ما يلي:
- العلاج غير الجراحي: العلاج غير الجراحي ممكن إذا كنت تعاني من أعراض خفيفة إلى معتدلة ولم تُظهر الفحوصات العصبية تلفًا كبيرًا في العصب المتوسط. قد تساعد الأدوية التي تحتوي على مضادات الالتهاب (مضادات الالتهاب غير الستيروئيدية) في تخفيف الألم الناتج عن متلازمة النفق الرسغي على المدى القصير فقط.
- الجبيرة الليلية (جبيرة المعصم): إن العلاج التحفظي الأكثر فعالية هو التجبير الليلي باستخدام جبيرة المعصم خصيصًا. إذا كنت تستخدمها، فتجنب ارتدائها طوال اليوم، لأن ذلك يمكن أن يضعف عضلات الرسغين واليدين. ومع ذلك، يوصى بارتدائها طوال الليل. يجب أن يتم ذلك لمدة 3 أشهر على الأقل.
- الجراحة: إذا استمرت الأعراض أو أصبحت سرعة التوصيل العصبي أسوأ، فيجب التفكير في الجراحة. يتم استخدام نوعين رئيسيين من الجراحة لتخفيف الضغط على الأعصاب داخل النفق الرسغي: جراحة تحرير النفق الرسغي المفتوحة وجراحة تحرير النفق الرسغي بالمنظار الأحدث. وكلاهما إجراءان يتم إجراؤهما في العيادات الخارجية تحت التخدير الموضعي (يقوم الجراح بقطع الرباط على طول منتصف الكف وداخل المعصم).
التغييرات في نمط الحياة والعلاجات المنزلية
قد توفر هذه الخطوات تخفيفًا مؤقتًا للأعراض:
- خذ فترات راحة قصيرة ومتكررة من الأنشطة المتكررة التي تنطوي على استخدام اليدين.
- إنقاص الوزن إذا كنت تعاني من زيادة الوزن أو السمنة.
- قم بتدوير الرسغين ومدّ الكفين والأصابع.
- تناول مسكنات الألم، مثل الأسبرين أو الأيبوبروفين (أدفيل أو موترين آي بي أو غيرهما) أو نابروكسين الصوديوم (أليف).
- ارتدِ جبيرة معصم مريحة وليست ضيقة ليلاً. يمكنك العثور عليها دون وصفة طبية في معظم متاجر الأدوية أو الصيدليات.
- تجنبي النوم على يديك.
إذا تكرر الألم أو الخدر أو الضعف واستمر، يُرجى مراجعة مقدم الرعاية.
الطب البديل
ادمج العلاجات البديلة في خطتك العلاجية لمساعدتك في التغلب على متلازمة النفق الرسغي. قد تضطر إلى التجربة للعثور على العلاج المناسب لك. استشر دائمًا مقدم الرعاية الخاص بك قبل تجربة أي علاج تكميلي أو بديل.
- اليوغا: قد تساعد وضعيات اليوغا المصممة لتقوية الجزء العلوي من الجسم والمفاصل وإطالة وتوازنها في تقليل الألم وتحسين قوة القبضة.
- علاج اليد: تشير الأبحاث المبكرة إلى أن بعض تقنيات العلاج الطبيعي والمهني لليدين قد تقلل من أعراض متلازمة النفق الرسغي.
- العلاج بالموجات فوق الصوتية: يمكن استخدام الموجات فوق الصوتية عالية الكثافة لرفع درجة حرارة المنطقة المستهدفة من أنسجة الجسم لتقليل الألم وتعزيز الشفاء. تُظهر الأبحاث نتائج غير متناسقة مع هذا العلاج، ولكن قد تساعد دورة العلاج بالموجات فوق الصوتية على مدار عدة أسابيع في تقليل الأعراض.
التعافي
يتعافى معظم الأشخاص بشكل كامل، ولكن في بعض الحالات (أقل من 5 في المئة) تتكرر متلازمة النفق الرسغي بعد الجراحة. ويحدث ذلك بشكل أكثر شيوعًا بعد إجراء التنظير الداخلي، والذي غالبًا لا يفتح النفق بشكل كامل مثل عملية التحرير المفتوحة.
الملخص
إذا كنت تعاني من أعراض متلازمة النفق الرسغي وتبحث عن أكثر أطباء الأعصاب خبرة لتشخيص الحالة وتقديم أفضل علاج، فإن المركز الألماني لطب الأعصاب هو عيادتك المفضلة. منذ أكثر من 15 عاماً والمركز الألماني لطب الأعصاب هو العيادة الرائدة في مجال طب الأعصاب في الإمارات العربية المتحدة. جميع خبراء النفق الرسغي لدينا حاصلون على شهادة البورد الألماني ولديهم خبرة مهنية لا تقل عن 25 عاماً. إذا كنت تبحث عن أكثر خبراء النفق الرسغي الموثوقين، فقد جئت إلى المكان الصحيح. احجز موعدك هنا
آلام الأعصاب وتلفها
العصب المضغوط، العصب المقروص، العصب المضغوط، العصب المضغوط، ألم العصب ثلاثي التوائم
قد تتعرض الأعصاب في مسارها التشريحي عبر الجسم والأطراف للتلف بطرق مختلفة، وغالباً ما يكون سبب التلف رضوضاً. وقد تتمثل أعراض تلف الأعصاب في الوخز والخدر والألم وكذلك الشلل أو اضطرابات المثانة أو المستقيم. تُعد آلام أسفل الظهر من أكثر الشكاوى شيوعاً اليوم. يعاني ما يصل إلى 80% من سكان الولايات المتحدة الأمريكية من آلام الظهر مرة واحدة على الأقل في حياتهم. آلام الظهر أو آلام أسفل الظهر هي أكبر سبب للغياب عن العمل في المملكة المتحدة.
ألم العصب الثلاثي التوائم
ألم العصب ثلاثي التوائم هو حالة خاصة من آلام الأعصاب. وغالباً ما يوصف بأنه "أسوأ ألم في العالم". وعادةً ما يعاني المرضى من نوبات من آلام الوجه الشديدة الشبيهة بالصدمة الكهربائية على طول العصب ثلاثي التوائم. المزيد من المعلومات هنا: ألم العصب ثلاثي التوائم
الأسباب وعوامل الخطر
غالباً ما تنحصر الأعصاب في الحبل الشوكي أو العمود الفقري أو في مسارها إلى الأطراف. وقد يكون السبب في ذلك بعض الإصابات، أو انزلاق غضروفي أو انحباس العصب في قناة عظمية أو قناة النسيج الضام. ومن الأمثلة النموذجية على ذلك متلازمة النفق الرسغي.
الأعراض
تعتمد الأعراض على موقع العصب المصاب أو التالف. في كثير من الأحيان يتم ضغط الأعصاب في عنق الرحم أو الظهر القطني بسبب انزلاق غضروفي مما يسبب آلام الرقبة أو الظهر والساق. وهناك موقع شائع آخر هو الرسغ. إذا تم ضغط العصب هنا ينتج عنه ألم في اليد يسمى متلازمة النفق الرسغي. ولكن يمكن أن تتسبب العديد من الحالات الأخرى في تلف الأعصاب في أماكن مختلفة مثل الإصابات الرياضية المتعلقة بالكتف وغيرها.
التشخيص
الأهم من ذلك هو استشارة طبيب أعصاب متمرس. يتم توجيه الانطباع السريري والفحص البدني. إذا تم تحديد الموقع، يمكن استخدام بعض اختبارات الأعصاب مثل سرعة توصيل العصب أو تخطيط كهربية العضل للتحقق من التشخيص أو لتحديد الموقع بدقة.

العلاج
يجب تجربة جميع خيارات العلاج التحفظي قبل التفكير في التدخل الجراحي. تعتمد خيارات العلاج هذه أيضاً على موقع العصب التالف أو المضغوط. غالباً ما يكون العلاج الطبيعي المتخصص وبعض الدعامات وتعديلات نمط الحياة ناجحة. وعلاوة على ذلك، فإن التحكم في الألم بشكل كافٍ والأدوية الأخرى ضرورية لتحسين الشفاء السريع. يمكن علاج معظم تلف الأعصاب بنجاح دون جراحة.
فريق الخبراء لدينا
منذ أكثر من عشر سنوات تعتبر GNC العيادة الرائدة في مجال طب الأعصاب في الإمارات العربية المتحدة. جميع خبراء تلف الأعصاب لدينا حاصلون على شهادة البورد الألماني ولديهم خبرة مهنية لا تقل عن 25 عاماً. إذا كنت تبحث عن أكثر خبراء تلف الأعصاب الموثوق بهم، فقد جئت إلى المكان الصحيح.
يمكننا أيضاً مساعدتك في الحصول على أفضل الأطباء النفسيين والأطباء النفسيين والمعالجين النفسيين المتاحين في دبي، الإمارات العربية المتحدة.Testimonials
``It was a great visit thanks! It really helped me.``
``Great service``
``God bless you guys wish you more of success``
``I'm impressed by the Professor and team professionalism``
``Being able to have blood tests and EEG done at the clinic itself was very helpful and convenient. This also allowed my doctor to have fast access to the test results.``
``I am thankful for the service.``
``Excellent doctor``
``The doctor is the best and everyone's very helpful``
As Seen On
التصلب المتعدد
- المرض
ما هو التصلب المتعدد؟
التصلب المتعدد (MS) هو اضطراب مناعي ذاتي يهاجم فيه الجهاز المناعي لجسمك الأعصاب وخاصةً أغلفة المايلين الخاصة بها. يؤدي تلف المايلين إلى تعطيل التواصل بين الخلايا العصبية. وبالتالي يمكن أن تتعطل الوظائف التي تتحكم فيها الأعصاب. ونظراً لأن الجهاز العصبي يتحكم في جميع وظائف جسم الإنسان تقريباً، فقد يظهر التصلب المتعدد من خلال أعراض مختلفة. ولهذا السبب يصعب تشخيص التصلب العصبي المتعدد ويستغرق أحياناً سنوات. وهو مرض لا يمكن التنبؤ به وغالباً ما يسبب الإعاقة ويحدث في المقام الأول لدى الشباب البالغين الذين تتراوح أعمارهم بين 20 و40 عاماً. ويشيع مرض التصلب العصبي المتعدد لدى النساء ضعف شيوعه لدى الرجال.
لا يُعرف سبب التصلب اللويحي المتعدد ولكن قد تلعب العوامل المؤهبة الخارجية والداخلية دورًا في الإصابة به. على الرغم من عدم وجود علاج لمرض التصلب اللويحي المتعدد يمكن أن تساعد العلاجات في تسريع التعافي من النوبات وتعديل مسار المرض والتحكم في الأعراض.
التصلب المتعدد وفيتامين د
يلعب فيتامين د دورًا في تنظيم الجهاز المناعي في جسم الإنسان. وبما أن التصلب المتعدد مرض مناعي، فقد يكون لفيتامين (د) تأثير وقائي/معدّل يؤثر على المرض بشكل إيجابي. read more
التصلب اللويحي في الإمارات العربية المتحدة | قلة التعرض للشمس؟
أظهرت دراسة أسترالية جديدة مرة أخرى الصلة بين قلة أشعة الشمس / نقص فيتامين د والتصلب المتعدد. ولكن هل لدينا أشعة شمس أقل من اللازم في الإمارات العربية المتحدة؟ يدرس الباحثون منذ عام 1974 (غولدبرغ) الصلة بين قلة ضوء الشمس والتصلب المتعدد.
التصلب المتعدد والتدخين
يمكن أن تُظهر الدراسات أن التدخين والتدخين السلبي من عوامل خطر الإصابة بمرض التصلب العصبي المتعدد. وعلاوة على ذلك، يكون تشخيص مرضى التصلب العصبي المتعدد أسوأ إذا كانوا مدخنين مقارنة بالمرضى غير المدخنين. علاوة على ذلك، فإن أدوية التصلب العصبي المتعدد لا تكون فعالة إذا كان المرضى يدخنون. خلاصة القول: توقف عن التدخين!
الأعراض
غالبًا ما يتميز التصلب المتعدد بمسار انتكاسي انتكاسي، حيث تظهر أعراض جديدة على مدار أيام أو أسابيع وعادةً ما تتحسن جزئيًا أو كليًا، تليها فترة هدوء قد تستمر لأشهر أو حتى سنوات.
تتنوع علامات وأعراض التصلب اللويحي المتعدد بواحد أو أكثر مما يلي:- عدم وضوح الرؤية، وفقدان البصر، وازدواج الرؤية، وألم خلف العين (التهاب العصب البصري) خطر الإصابة بمرض التصلب العصبي المتعدد خلال الـ 15 سنة القادمة هو 50%!
- الاضطرابات الحسية، والخدر، والوخز، والألم
- ضعف في الأطراف، ومشاكل في المشي، وعدم التناسق، وعسر التلفظ، ورعاش النية
- خلل في المثانة أو الأمعاء
- تلعثم في الكلام
- الدوخة
- الإرهاق
التشخيص
قد يكون من الصعب تشخيص المراحل المبكرة من التصلب المتعدد. يمكن أن تظهر أعراض التصلب المتعدد من خلال مجموعة متنوعة من الأمراض الأخرى أيضًا. يجب إجراء فحص عصبي شامل من أجل استبعاد الحالات الأخرى التي قد تنتج عنها علامات وأعراض مشابهة. يتضمن الفحص اختبارات الدم وتصوير الرنين المغناطيسي للدماغ والعمود الفقري والبزل الشوكي (البزل القطني) الذي يتم فيه إزالة عينة صغيرة من السائل من القناة الشوكية لتحليلها في المختبر. يمكن أن تُظهر هذه العينة تشوهات في خلايا الدم البيضاء أو الأجسام المضادة المرتبطة بالتصلب المتعدد. علاوة على ذلك، سيتحقق طبيب الأعصاب من القوة الحركية والإحساس في جميع الأطراف.
العلاج
يعد علاج التصلب المتعدد مهمًا للغاية على الرغم من أن التصلب المتعدد مرض مزمن وموهن ولا يوجد له علاج. يركز العلاج على تقليل تواتر الانتكاسات وتسريع التعافي منها. والهدف من ذلك هو إبطاء تطور المرض والسيطرة على الأعراض. يجب تنسيق العلاج بالتشاور مع طبيب أعصاب متخصص في مرض التصلب العصبي المتعدد.
هناك أدوية خاصة لعلاج النوبات الحادة التي تقلل من التهاب الأعصاب. يمكن للأدوية الأخرى أن تقلل من معدل الانتكاس وتقلل من معدل تكوين آفات جديدة. وقد تمت الموافقة مؤخراً على أدوية جديدة لعلاج التصلب المتعدد.
إلى جانب ضرورة استخدام الأدوية المناسبة من أجل تخفيف الأعراض مثل الشلل والآلام واضطرابات الرؤية والعمى وغيرها من الأعراض العصبية، هناك أيضاً العلاج الطبيعي والتدابير العلاجية الأخرى التي يمكن أن تكون مفيدة. ومع ذلك، يعاني بعض المرضى من أعراض خفيفة بحيث لا يكون العلاج ضرورياً.
التعايش مع التصلب المتعدد
للتخفيف من علامات وأعراض التصلب المتعدد يجب أن يحاول المريض الحصول على قسط وافر من الراحة والاسترخاء. قد يساعد التأمل و/أو التنفس العميق. وعلاوة على ذلك، يمكن أن تساعد التمارين المنتظمة في تحسين القوة وتناغم العضلات والتوازن والتنسيق. تُعد السباحة والمشي وتمارين الإطالة والتمارين الرياضية منخفضة التأثير وركوب الدراجات الهوائية الثابتة واليوغا والتاي تشي من التمارين الخفيفة إلى المعتدلة الموصى بها لمرض التصلب العصبي المتعدد. تخفف التمارين أيضًا من التوتر الذي قد يؤدي إلى ظهور العلامات والأعراض أو تفاقمها. قد يكون من المفيد أيضًا اتباع نظام غذائي متوازن منخفض الدهون المشبعة ولكنه غني بالأحماض الدهنية أوميغا 3، مثل تلك الموجودة في زيوت الزيتون وزيت السمك. تشير الدراسات أيضًا إلى أن فيتامين د قد يكون له فوائد محتملة لمرض التصلب العصبي المتعدد.
إذا كنت تعتقد أنك تريد إصلاح شيء آخر يتعلق بصحتك العقلية. يوفر لك GNC دبي أحد أفضل الأطباء النفسيين في دبي والأطباء النفسيين في دبي والمعالجين النفسيين في دبي الذين يمكنهم مساعدتك في العثور على السبب الأساسي وفي إصلاحه.
مجموعة دعم مرض التصلب العصبي المتعدد في دبي
أنا مصاب بالتصلب المتعدد ولكن هل أبدو خائفاً؟
شابة مصابة بالمرض المنهك تطلق منتدى لمساعدة زملائها المرضى بدعم من المركز الألماني لعلوم الأعصاب، تطلق الشابة مها عباس البالغة من العمر ثمانية وعشرين عاماً والمصابة بمرض التصلب المتعدد منتدى "حوارات التصلب المتعدد" في مطعم "أوربان بيسترو" في دبي نهاية الشهر الجاري للتوعية بالمرض XPRESS، 14 أكتوبر 2015، شارميلا دال، رئيسة المراسلين في دبي: مها عباس، 28 عاماً، هي مريضة بالتصلب المتعدد (التصلب المتعدد) مع اختلاف.- المرض
إصابات الدماغ الرضحية (TBI)
إصابة الدماغ الرضحية (TBI) هي نتيجة لإصابة في الرأس حيث تؤدي الضربة على الرأس إلى تلف في الدماغ بسبب قوى التمدد. وتُعد الإصابة الدماغية الرضحية هي السبب الرئيسي للوفاة في أمريكا الشمالية للأشخاص الذين تقل أعمارهم عن 45 عاماً. وتتميز دولة الإمارات العربية المتحدة بصغر سن سكانها، مما يجعل الإصابة الدماغية الرضحية مرضاً شائعاً وخطيراً.
ويعيش العديد من الناجين مع إعاقات كبيرة، مما يؤدي إلى عبء اجتماعي واقتصادي كبير أيضاً. في عام 2000، قُدِّر الأثر الاقتصادي للإصابة بإصابات الرأس في الولايات المتحدة الأمريكية ب 9.2 مليار دولار أمريكي في التكاليف الطبية مدى الحياة و51.2 مليار دولار أمريكي في خسائر الإنتاجية.
غالبًا ما تكون الأعراض خفيفة ويصعب اكتشافها. تحتاج إلى أخصائي مدرب لتشخيص الحالة والأهم من ذلك علاجها. إذا عولجت الإصابة بالصدمة الدماغية التاجية بشكل كافٍ فإن تشخيصها جيد جداً.
الأسباب
- حوادث السيارات
- الإصابات الرياضية
- الإصابات الرياضية - السقوط
- العنف
- القتال العسكريالأعراض
إصابة الدماغ هي إصابة يساء فهمها في كثير من الأحيان. يتم تصنيف العديد من الشكاوى المتبقية غير المرئية على أنها "نفسية" وهي غير مفهومة جيداً. ومن الشكاوى الرئيسية لإصابة الدماغ الإرهاق والإفراط في التحفيز.
التحفيز الزائد
نحن نعيش في مجتمع سريع جدًا، حيث تتم معالجة الكثير من المحفزات بسرعة عالية. عندما يعاني الشخص من التحفيز الزائد، يصعب عليه معالجة المحفزات، حيث يُنظر إلى الأصوات على أنها أعلى والضوء على أنه أكثر سطوعاً. كما يُنظر إلى الضوضاء المحيطة على أنها مزعجة، ويصعب تحمل ضوء الشمس العادي، ويصبح من السهل على المرء أن يشعر بالارتباك بسبب الزحام وكثرة الحركات في محيطه.
الإرهاق
بسبب سرعة ظهور التعب، قد يكون من الصعب الذهاب إلى حفلات أعياد الميلاد والذهاب للتسوق من البقالة والمشاركة في الأنشطة الاجتماعية. يسبب التعب اضطرابات في عمليات التفكير ويحد من الأداء الوظيفي بالكامل. بعد قراءة نص ما، يمكن أن يكون المرء متعبًا بالفعل لدرجة أنه يجب أن يستريح لفترة من الوقت للتعافي من الجهد الذهني. على وجه الخصوص، يمكن أن تكون قراءة شاشات العرض (الهاتف الذكي، الكمبيوتر، الكمبيوتر اللوحي) مزعجة للغاية للمرضى الذين يعانون من إصابات الدماغ. وبالإضافة إلى الإرهاق والإفراط في التحفيز يلاحظ المرء أنه يواجه صعوبة أكبر في التذكر والتركيز. تصبح الذاكرة والتركيز أكثر صعوبة عند زيادة التعب.
الأعراض الثانوية
عندما يعاني المرء من الأعراض ولكنه يستمر في العمل بشكل يفوق قدراته، يمكن أن يصاب الناس بشكاوى ثانوية. لا يمكن مقارنة التحفيز المفرط للدماغ بالتحفيز المفرط للجسم. فالجسم لديه على سبيل المثال إشارات الألم كإشارة تحذير. أما الدماغ فيعطي إشارات تحذيرية مختلفة تماماً مثل التحفيز الزائد بسبب الضوء أو الضوضاء أو الازدحام، وصعوبة معالجة المنبهات، والمزيد من المشاكل في التفكير (التركيز والذاكرة) والإرهاق. لا يتعرف الكثير من الناس على إشارات الإنذار هذه، أو لا يتعاملون معها بشكل كافٍ ومن المرجح أن يدفعهم ذلك إلى تجاوز شكواهم. سيؤدي العمل خارج قدراتهم الخاصة إلى زيادة الشكاوى وفي النهاية سيحدث الإنهاك. كما أن عدم القدرة على العمل بالطريقة التي يرغب فيها المريض، يمكن أن يتطور لدى المريض ردود فعل عاطفية تتسم غالبًا بمشاعر العجز والإحباط. وبالتالي تتكون الإصابة غير المفهومة من الإرهاق والإجهاد، وسرعان ما يصبح المريض مرهقًا ويواجه انخفاضًا في الأداء والاستجابات العاطفية.
التشخيص الخاطئ لإصابات الدماغ الرضحية
غالباً ما يتم تشخيص مرضى إصابات الدماغ بشكل خاطئ أو لا يتم تشخيصهم على الإطلاق. ونظراً لأن معظم المهنيين غير متخصصين في تشخيص إصابات الدماغ، غالباً ما يسمع المرضى عبارة "لا يوجد شيء خاطئ"، حتى لو كانوا يعانون من أعراض. أو يتم تقييم أعراضهم على أنها "نفسية فقط". يؤدي عدم علاج الإصابة بالإصابة بإصابات الرضح النصفي بشكل كافٍ إلى تفاقم الأعراض. وتؤدي هذه العملية الموصوفة إلى عبء اجتماعي واقتصادي كبير (الولايات المتحدة: 9.2 مليار دولار أمريكي في التكاليف الطبية مدى الحياة و51.2 مليار دولار أمريكي في خسائر الإنتاجية).
التشخيص
التقييم النفسي العصبي ضروري للحصول على انطباع جيد عن الأعراض المتبقية "غير المرئية" وكيفية التعامل معها. يُستخدم الفحص النفسي العصبي لتقييم مدى فقدان الطاقة (الذهنية) والإرهاق والتغيرات الإدراكية - / العاطفية وتأثير الإحساس بالألم.
في بداية الاستشارة/العلاج، يتم إجراء مقابلة مطولة (أناميس) مع المريض. تتم مناقشة مجموعة واسعة من القضايا، مثل ما الذي حدث، وما هي الأعراض، وهل كانت نقطة الانهيار في الإدراك الصحي، وما هي الظروف التي تزيد من تفاقم الأعراض أو تؤثر عليها. وعلاوة على ذلك، ننظر في التاريخ (الطبي) والتعليم ونوع العمل والهوايات والحياة الاجتماعية وكيف تحد الشكاوى من ذلك. يتم إجراء فحص نفسي عصبي وعلى أساس النتائج يتم اقتراح خطة علاجية مناسبة. في حالة عدم توفر معلومات كافية، يمكن استشارة خبرات العديد من التخصصات الأخرى (أطباء الأعصاب، أطباء الباطنية، الأطباء النفسيين، إلخ).
من خلال هذه المعلومات والفهم، من الممكن إنشاء علاج مناسب يشمل الأشخاص الذين يعانون من إصابات الدماغ لفهم القيود الفعلية وكيفية التكيف معها.
العلاج
من المهم معرفة أن المرضى أنفسهم غالباً ما لا يكون لديهم فهم جيد لمحدودية الأعراض والشكاوى التي يعانون منها، ويُدفع المريض إلى الأداء بمستوى ما قبل المرض. يعد التعافي من تلف الدماغ عملية معقدة يجب أن يمر بها المريض بمساعدة متخصص. من الضروري أن يكتسب المرء المعرفة في عرض الأعراض ويحصل أيضاً على المشورة في كيفية التعامل معها. إصابة الدماغ هي في الأساس ظاهرة نفسية عصبية.
إعادة التأهيل النفسي العصبي
في المرحلة التالية، يتم إعادة تنشيط الوظائف الإدراكية المصابة واستخدام برنامج لياقة طبية لتحسين مستوى الطاقة وتقليل مستويات الألم.
في كثير من الأحيان، يتكون العلاج من إرشادات أخصائي علم النفس العصبي السريري الذي سيقدم نظرة ثاقبة للشكاوى وسبب حدوثها. يتم تدريس التعديلات ومناقشة جداول التمارين/الراحة. خلال نفس الفترة، سيتبع المرضى برامج اللياقة الطبية وبرنامج التدريب الإدراكي. يلي ذلك فترات راحة. إذا ظلت أعراض الألم واضحة، يتم اللجوء إلى طبيب الأعصاب أو طبيب الألم (طبيب التخدير). وغالباً ما يتكون الإحساس بالألم من ألم في الرقبة والكتفين والذي يتطور أيضاً إلى صداع. تتم مناقشة تقدم كل مريض يومياً ويتم تكييف البرامج مع هذه الملاحظات. الهدف هو أن يصبح الفرد متوازنًا بشكل جيد مرة أخرى.
ولتحقيق ذلك، ينصب التركيز الرئيسي على الاهتمام الشخصي. وجهة نظرنا هي أن كل شخص يشبه بصمة الإصبع، فهو فريد من نوعه تماماً. لا يوجد بروتوكول قياسي يُستخدم لتقديم العلاج، حيث أن لكل شخص طريقته الخاصة في التفاعل مع جميع الجوانب المتعلقة بإصابة الدماغ.
مدة البرنامج عادةً ثلاثة أشهر والحد الأقصى لحجم المجموعة هو 12 شخصاً. الهدف الرئيسي للمجموعة الصغيرة هو بناء علاقة شخصية مع كل مشارك في البرنامج.
إذا كنت تعتقد أنك تريد إصلاح شيء آخر يتعلق بصحتك النفسية. يوفر لك مركز دبي الوطني للأطباء النفسيين في دبي أحد أفضل الأطباء النفسيين في دبي والأطباء النفسيين في دبي والمعالجين النفسيين في دبي الذين يمكنهم مساعدتك في العثور على السبب الأساسي وفي إصلاحه.
المفهوم الخاطئ الشائع
غالبًا ما يكون هناك اعتقاد خاطئ بأن شكاوى إصابات الدماغ (الخفيفة) ستزول بعد مرور بعض الوقت. لا يمكن أن يحدث هذا التعافي الطبيعي إلا عندما تكون الظروف مثالية. يحتاج المرء إلى أداء الأنشطة المناسبة خلال فترة التعافي من أجل تحسين التعافي. وتجدر الإشارة إلى أنه حتى مع فترة التعافي المثلى قد تكون هناك شكاوى متبقية!
مرض باركنسون
Disease
ما هو مرض باركنسون؟
داء باركنسون هو اضطراب عصبي تنكسي تدريجي يتميز بالتصلب والرعشة وعدم استقرار الوضعية وبطء الحركة. يتطور المرض تدريجياً، ويبدأ أحياناً برعشة بالكاد يمكن ملاحظتها في يد واحدة فقط. وغالباً ما تكون التغييرات في الحركة غير ملحوظة للغاية وبالتالي غالباً ما يكون التشخيص المبكر صعباً. يسبب المرض عادةً تصلباً أو تباطؤاً في الحركة. على الرغم من عدم إمكانية الشفاء من مرض باركنسون، إلا أن الأدوية قد تُحسّن الأعراض بشكل ملحوظ.

المرض
الأعراض
قد تكون أعراض مرض باركنسون خفيفة في البداية وغالبًا ما تبدأ في جانب واحد من الجسم. قد تشمل العلامات والأعراض ما يلي:
- الرعشة (رعشة اليدين)
- تباطؤ الحركة
- تيبس العضلات
- ضعف الوضعية والتوازن
- فقدان الحركات التلقائية
- مشاكل النطق والكتابة
قد تكون هناك أعراض أخرى مثل انخفاض وظائف الدماغ الفكرية العليا، وأعراض نفسية مثل الاكتئاب وكذلك اضطرابات في وظائف الجسم النباتية.

المرض
الأسباب
في مرض باركنسون، تنهار أو تموت تدريجياً خلايا عصبية معينة (خلايا عصبية) في الدماغ. هذه الخلايا العصبية المعينة هي المسؤولة عن تصميم وتطوير وتحقيق الحركات. يؤدي فقدان الخلايا العصبية إلى انخفاض مستوى الدوبا في الدماغ. الدوبا هو ناقل كيميائي بين الخلايا العصبية. لا تُعرف أسباب مرض باركنسون ولكن قد تلعب عوامل مثل الجينات والمحفزات البيئية دوراً في الإصابة بالمرض. ومع ذلك، فإن الرجال أكثر عرضة للإصابة بالمرض من النساء وعادة ما يبدأ المرض في سن الستين أو أكثر.
التشخيص
قد يكون التشخيص المبكر لمرض باركنسون صعباً لأن الأعراض غالباً ما تكون خفية. سيقوم طبيب الأعصاب بفحص شامل للتاريخ المرضي والفحص البدني ويطلب إجراء فحوصات لاستبعاد الحالات الأخرى التي قد تكون سبباً في ظهور الأعراض. بالإضافة إلى ذلك، قد يعطي دواءً معيناً لمرض باركنسون. غالباً ما يؤكد التحسن الملحوظ مع هذا الدواء تشخيص مرض باركنسون.
العلاج
حتى الآن، لا يوجد علاج لمرض باركنسون ولكن بعض الأدوية يمكن أن تساعد في السيطرة على الأعراض. يمكن أن تساعد في السيطرة على مشاكل المشي والحركة والرعاش عن طريق زيادة إمدادات الدماغ من الدوبا. واعتماداً على مرحلة مرض باركنسون وعمر المريض، يتم وصف أدوية مختلفة. بعض الأدوية لها تأثير محدود لبضع سنوات فقط. إذا لم يعد التأثير كافياً بعد الآن يجب زيادة الدواء أو تغييره.
سيكون التركيز الرئيسي للعلاج على الأدوية المناسبة والعلاج الطبيعي. تعتبر التمارين البدنية من الوسائل العلاجية المفيدة. في الحالات الشديدة قد يكون التدخل الجراحي العصبي ضرورياً وهو ما يُعرف بالتحفيز العميق للدماغ. يقوم الجراحون بزرع أقطاب كهربائية في جزء معين من الدماغ وتوصيلها بمولد مزروع في الصدر بالقرب من عظمة الترقوة يرسل نبضات كهربائية إلى الدماغ. قد يقلل التحفيز العميق للدماغ من أعراض مرض باركنسون.
التعايش مع مرض باركنسون
من الضروري أن يعمل المريض عن كثب مع طبيب الأعصاب لإيجاد العلاج المناسب. قد تساعد بعض التغييرات في نمط الحياة مثل اتباع نظام غذائي صحي وممارسة التمارين البدنية في تسهيل التعايش مع مرض باركنسون. يوصى بالمشي أو السباحة أو الرقص أو التمارين الرياضية المائية أو تمارين الإطالة من أجل تحسين التوازن الذي قد يختل بسبب المرض. وعلاوة على ذلك، يمكن أن تكون بعض أنواع الطب البديل مثل التأمل واليوغا والتدليك والتاي تشي والوخز بالإبر الصينية أدوات مفيدة.
يمكننا أيضاً مساعدتك في الحصول على أفضل الأطباء النفسيين والأطباء النفسيين والمعالجين النفسيين المتوفرين في دبي، الإمارات العربية المتحدة.
© GNC, German Neuroscience Center Dubai (Neurology, Psychiatry, Psychology, Counseling, Dubai, UAE)
الاعتلال العصبي السكري
الاعتلال العصبي - الاعتلال العصبي المتعدد الأعصاب
الاعتلال العصبي هو مصطلح يصف تلف الأعصاب. تشمل الأعراض الأكثر شيوعاً: الألم (غالباً ما يكون أسوأ في الليل)، والخدر، والوخز، و"الوخز والإبر"، والإحساس بالحرقان، وضعف العضلات وغيرها. يمكن أن يكون الضرر ناتجاً عن حالات مختلفة مثل المرض أو العدوى أو الإصابة أو الأدوية أو السموم أو أي سبب آخر.
أنواع الاعتلال العصبي
- يؤثر الاعتلال العصبي المحيطي على الأعصاب في الأجزاء الخارجية (الطرفية) من الجسم مثل القدمين والساقين واليدين والذراعين.
- يؤثر الاعتلال العصبي الداني على عضلات الوركين والكتفين.
- يؤثر الاعتلال البؤري أو أحادي العصب على عصب واحد فقط. مثال على ذلك متلازمة النفق الرسغي.
- يؤثر اعتلال الأعصاب المتعدد على العديد من الأعصاب. معظم المصابين باعتلال الأعصاب لديهم اعتلال الأعصاب المتعدد.
- الاعتلال العصبي اللاإرادي: تتضرر أعصاب الجهاز العصبي اللاإرادي مما يؤدي إلى أعراض مثل مشاكل في الهضم وضغط الدم ووظيفة المثانة.
- يؤثر الاعتلال العصبي السكري الناجم عن داء السكري بشكل شائع على أعصاب اليدين والقدمين. كما يمكن أن يؤثر أيضاً على الأعصاب التي تتحكم في الوظائف التلقائية للجسم، مثل الهضم، أو أعصاب الوركين والفخذين.
اعتلال الأعصاب السكري في الإمارات العربية المتحدة هو النوع الأكثر شيوعاً. لذلك، سنصف هذا النوع أدناه بشكل أكثر استفاضة.
الاعتلال العصبي السكري
يعاني 60-70% من مرضى السكري من اعتلال الأعصاب السكري. قد يكون الاعتلال العصبي موجوداً حتى قبل تشخيص مرض السكري. مرض السكري هو السبب الأكثر شيوعاً للاعتلال العص بي المحيطي في العالم. ومع ذلك، فإن أعراض الاعتلال العصبي غير معروفة في الغالب للمرضى ويصعب تشخيصها. التشخيص المبكر مهم لأن الاعتلال العصبيالسكري يمكن أن يتلف أي عصب في جسم الإنسان. سواء كانت الأعصاب التي تتحكم في نبضات القلب أو أعصاب الجلد. تعد الآفات الجلدية الناتجة عن مرض السكري السبب الرئيسي لبتر القدم.
الأسباب
على غرار تنوع الأعراض، هناك أيضًا مجموعة كبيرة ومتنوعة من الأسباب لهذا المرض. السبب الأكثر شيوعاً هو اضطراب التمثيل الغذائي مثل داء السكري. ولكن أيضاً يمكن أن يتسبب التصرف الوراثي أو تثبيط السموم أو تطور الأباعد الورمية في حدوث اعتلال الأعصاب.
العلامات والأعراض
إن الاعتلال العصبي السكري يعني إصابة العديد من الأعصاب لأسباب مختلفة جداً وبالتالي يمكن أن تظهر العديد من الأعراض المختلفة. والأكثر شيوعًا هي الإصابة بشبه الحساسية مثل الوخز والخدر وحرقان القدمين، وكذلك الشلل واضطرابات النطق وفشل الأعصاب الدماغية.
أنواع الاعتلال العصبي السكري
هناك أنواع مختلفة من الاعتلال العصبي مع أنماط نموذجية مختلفة لتوزيع الألم. على سبيل المثال هناك
قراءة المزيد
العلاج
وبناءً على ذلك، فإن تشخيص وعلاج اعتلال الأعصاب المتعدد متعدد الأعصاب متعدد الأعصاب متعدد الجوانب وصعب. يجب أن يكون الهدف العلاجي هو منع تدهور الأعصاب نفسها من ناحية، وعلاج الأمراض المسببة لاعتلال الأعصاب المتعددة من ناحية أخرى. إن أهم الأجزاء الأساسية في تقييم التشخيص والعلاج هي...
قراءة المزيد
فريق الخبراء لدينا
منذ أكثر من عشر سنوات تعتبر GNC العيادة الرائدة في مجال طب الأعصاب في الإمارات العربية المتحدة. جميع خبراء الاعتلال العصبي لدينا حاصلون على شهادة البورد الألماني ولديهم خبرة مهنية لا تقل عن 25 عاماً. إذا كنت تبحث عن خبراء الاعتلال العصبي الأكثر ثقة، فقد جئت إلى المكان الصحيح.
متلازمة تململ الساقين
المرض
ما هي متلازمة تململ الساقين؟
متلازمة تململ الساقين (RLS) هي اضطراب عصبي يتميز بشعور مزعج للغاية مثل الزحف أو الخفقان أو الشد أو الحكة أو الإبر والدبابيس في الساقين، وعادةً ما يكون ذلك في المساء أثناء الجلوس أو الاستلقاء. يجعل المريض يشعر بالرغبة في النهوض والتحرك مما يخفف من الشعور المزعج مؤقتاً. تؤثر متلازمة تململ الساقين في الغالب على الساقين، ولكن يمكن أن تؤثر أيضاً على الذراعين والجذع والرأس وحتى الأطراف الوهمية. يمكن أن يعطل النوم وبالتالي يؤدي إلى النعاس أثناء النهار.
غالبًا ما تبدأ أعراض متلازمة تململ الساقين المتقطع في سن الأربعين من العمر، ولكن ما يصل إلى ثلث المرضى تظهر عليهم الأعراض قبل سن العشرين. وتصيب متلازمة متلازمة متلازمة تململ الساقين المتقطع ما بين 7 إلى 10% من الشباب ومتوسطي العمر، وما بين 10% إلى 20% ممن تزيد أعمارهم عن 60 عاماً. في منطقة الشرق الأوسط يصاب به حوالي 3% من عامة السكان. ويصيب النساء أكثر بمرتين من الرجال. وتعاني النساء الحوامل على وجه الخصوص من متلازمة تململ الساقين. وتصاب 25% من النساء الحوامل بهذا الاضطراب في الأشهر الثلاثة الأخيرة من الحمل.
الأعراض
تتواجد أعراض متلازمة تململ الساقين بشكل شائع في أعماق الساقين والقدمين والفخذين. في البداية غالباً ما يشعر المريض في البداية بإحساس مبالغ فيه بالوعي الموضعي للساق المصابة، وتظهر الأحاسيس أو تشتد لاحقاً حتى أثناء الجلوس. تجلب حركة الجزء المصاب من الجسم، مثل المشي على سبيل المثال، راحة فورية، على الرغم من أنها مؤقتة وجزئية وتعود الأحاسيس مباشرة بعد توقف الحركة. وغالباً ما تؤدي هذه الأعراض إلى نقص حاد في النوم مع تعب ثانوي وفقدان التركيز في العمل أو أثناء قيادة السيارة. بعض الأشخاص الذين يعانون من متلازمة متلازمة تململ الساقين الحادة لا يستطيعون حتى الذهاب إلى العمل.
الأسباب
يُميّز المرء بين نوعين من متلازمة تململ الساقين: متلازمة تململ الساقين الأولية والثانوية.
متلازمة متلازمة تململ الساقين الأولية (مجهولة السبب) هي مرض عصبي غير معروف الأسباب. يُشتبه في وجود اضطراب في نظام الناقل العصبي في الدماغ. تساعد الأدوية التي تتداخل مع نظام الناقل العصبي بشكل موثوق.
وترتبط متلازمة تململ الساقين الثانوي (الأعراض) في الغالب بنقص الحديد أو الاضطرابات الوريدية أو اعتلال الأعصاب أو نقص الفولاسيت أو السكري أو أمراض الكلى أو الحمل.
يمكن أيضًا أن تحدث متلازمة تململ الساقين بسبب الأدوية المضادة للقىء ومضادات الاكتئاب ومضادات الذهان. لا ينبغي النظر في متلازمة تململ الساقين الأولي حتى يتم استبعاد الحالات الطبية المحتملة، خاصةً الاضطرابات الوريدية واعتلال الأعصاب.
عوامل الخطر
- العمر. تصيب المتلازمة 10 في المائة من الأشخاص الذين تبلغ أعمارهم 65 عامًا فأكثر، مقارنة بـ 5 في المائة فقط من عامة السكان.
- الجنس. النساء أكثر عرضة للإصابة بهذه الحالة من الرجال، ولكن يبدو أن العلاقة بين الجنسين مرتبطة بالحمل. إذا لم تكن المرأة حاملاً من قبل، فإن خطر إصابتها بالمرض هو نفس خطر إصابة الرجل.
- نقص الحديد. يرتبط نقص الحديد في الدماغ بالمتلازمة.
- التاريخ العائلي. يكون الأشخاص الذين لديهم تاريخ عائلي للمرض أكثر عرضة للإصابة بالمرض.
أكثر من مجرد إزعاج
اكتشف باحثون من جامعة هارفارد أن الحرمان من النوم - الناجم عن متلازمة تململ الساقين (RLS) - يؤدي إلى ارتفاع خطر الوفاة المبكرة. وقد ربطت دراسات سابقة بين متلازمة تململ الساقين (RLS) والعديد من الحالات الأخرى، بما في ذلك الاكتئاب وارتفاع ضغط الدم وأمراض القلب. وهذا يدل على أن متلازمة تململ الساقين ليست مجرد إزعاج أو حالة تسبب مشاكل في النوم. بل لها آثار شديدة على الصحة العامة وطول العمر.
العلاج
الهدف من علاج متلازمة تململ الساقين هو تقليل الأحاسيس غير المريحة. في بعض الأحيان يكون من الضروري علاج الحالات الكامنة مثل نقص الحديد أو الاعتلال العصبي المحيطي.
مع الدواء
لتقليل الأرق في الساقين هناك العديد من الأدوية المتوفرة مثل أدوية مرض باركنسون التي تقلل من كمية الحركة في الساقين من خلال التأثير على مستوى الناقل العصبي في الدماغ. وعلاوة على ذلك، قد تساعد أدوية الصرع في تقليل الشعور بعدم الارتياح، بالإضافة إلى أدوية إرخاء العضلات وأدوية النوم. لكن هذه الأدوية لا تقضي على الإحساس بالساقين، وقد تسبب النعاس أثناء النهار.
بدون دواء
يلعب الحديد دوراً كبيراً في متلازمة تململ الساقين. يجب قياس مستويات الحديد وموازنة نقصه. وعلاوة على ذلك، يشمل العلاج غير الطبي تجنب الكافيين والكحول والنيكوتين والأدوية التي تؤدي إلى تفاقم متلازمة تململ الساقين والنشاط البدني والنظافة الصحية الجيدة للنوم. غالباً ما تلعب التغييرات البسيطة في نمط الحياة دوراً مهماً في التخفيف من أعراض متلازمة تململ الساقين وتعلم بعض تقنيات الاسترخاء مثل اليوغا والتأمل يمكن أن يؤدي إلى تحسن كبير.
© GNC, German Neuroscience Center Dubai (Neurology, Psychiatry, Psychology, Counseling, Dubai, UAE)
التصلب الجانبي الضموري (ALS)
التصلب الجانبي الضموري الضموري (ALS)، المعروف باسم مرض لو جيريج، هو اضطراب عصبي متقدم يؤثر على الخلايا العصبية في الدماغ والحبل الشوكي. نحن في المركز الألماني لعلوم الأعصاب بدبي ملتزمون بتوفير معلومات شاملة عن التصلب الجانبي الضموري لمساعدة المرضى وعائلاتهم على فهم هذه الحالة بشكل أفضل. في هذه المقالة، سنتناول في هذه المقالة العلامات وعوامل الخطر والتشخيص والعلاجات وغيرها من المعلومات ذات الصلة لتمكين المرضى الذين يواجهون التصلب الجانبي الضموري.
أعراض التصلب الجانبي الضموري (ALS)
يستهدف التصلب الجانبي الضموري الضموري في المقام الأول الخلايا العصبية الحركية المسؤولة عن حركة العضلات، مما يؤدي إلى مجموعة من الأعراض التي تتفاقم تدريجيًا بمرور الوقت. تشمل الأعراض المبكرة الشائعة ضعف العضلات والوخز والتشنجات، وغالبًا ما تكون في الذراعين أو الساقين. مع تقدم التصلب الجانبي الضموري الضموري قد يعاني المرضى من صعوبة في الكلام والبلع والتنفس. يُعد ضمور العضلات وفقدان التحكم الحركي من السمات المميزة للمرض، مما قد يتسبب في صعوبات في الحركة ويؤثر على الحياة اليومية.
عوامل خطر الإصابة بالتصلب الجانبي الضموري (ALS)
في حين أن السبب الدقيق للتصلب الجانبي الضموري الضموري لا يزال غير معروف، فقد تم تحديد بعض عوامل الخطر. على الرغم من أن التصلب الجانبي الضموري الضموري يمكن أن يصيب أي شخص، إلا أنه أكثر شيوعًا في الأفراد الذين تتراوح أعمارهم بين 40 و70 عامًا. قد تلعب العوامل الوراثية دورًا أيضًا، حيث تكون نسبة صغيرة من الحالات عائلية. كما تم ربط العوامل البيئية، مثل التعرض للسموم أو الإصابات المؤلمة، بزيادة خطر الإصابة بالتصلب الجانبي الضموري.
التشخيص
يتطلب تشخيص مرض التصلب الجانبي الضموري الضموري تقييماً شاملاً، وغالباً ما يتضمن العديد من الفحوصات الطبية. تساعد الفحوصات العصبية وتخطيط كهربية العضل (EMG) لتقييم نشاط العضلات ودراسات التوصيل العصبي على تحديد الأنماط المميزة لخلل وظيفي في الخلايا العصبية الحركية. بالإضافة إلى ذلك، يمكن أن يستبعد التصوير بالرنين المغناطيسي وتقنيات التصوير الأخرى الأسباب المحتملة الأخرى للأعراض.
علاجات التصلب الجانبي الضموري (ALS)
في حين أنه لا يوجد علاج لمرض التصلب الجانبي الضموري الضموري (ALS)، يمكن أن يساعد النهج متعدد التخصصات في إدارة الأعراض وتحسين جودة الحياة وتوفير الرعاية الداعمة. قد تؤدي بعض الأدوية إلى إبطاء تقدم المرض وتحسين متوسط العمر المتوقع. يمكن أن يساعد العلاج الطبيعي والعلاج الوظيفي وعلاج النطق في الحفاظ على وظيفة العضلات ومعالجة تحديات الحركة. كما تلعب الأجهزة المساعدة والتقنيات التكيفية دوراً محورياً في تعزيز الاستقلالية والتواصل.
الرعاية الداعمة والأبحاث
يستفيد مرضى التصلب الجانبي الضموري الضموري من الرعاية المستمرة لتلبية الاحتياجات المتطورة للمرض. تقدم مجموعات الدعم والاستشارات الدعم العاطفي والنفسي للمرضى وعائلاتهم، مما يساعدهم على التغلب على التحديات التي يمثلها التصلب الجانبي الضموري. يشارك المركز الألماني لعلوم الأعصاب في دبي بنشاط في المبادرات الرامية إلى تطوير فهمنا لمرض التصلب الجانبي الضموري مما يؤدي إلى تحسين خيارات العلاج والتقدم المحتمل.
الخاتمة
التصلب الجانبي الضموري هو اضطراب عصبي معقد يتطلب إدارة ودعم شاملين. في المركز الألماني لعلوم الأعصاب بدبي، نلتزم في المركز بتزويد المرضى بأحدث المعلومات والرعاية الشخصية لمساعدتهم على مواجهة التحديات التي يفرضها التصلب الجانبي الضموري. من خلال فهم الأعراض وعوامل الخطورة والتشخيص والعلاجات والجهود البحثية المستمرة، يمكن للمرضى وعائلاتهم اتخاذ قرارات مستنيرة وتلقي الدعم الذي يحتاجونه في رحلتهم مع التصلب الجانبي الضموري. اتصل بنا اليوم لمعرفة المزيد عن خدماتنا وكيف يمكننا مساعدتك في التعامل مع مرض التصلب الجانبي الضموري بفعالية.
الوهن العضلي الوبيل
الوهن العضلي الوبيل
الوهن العضلي الوبيل هو مرض مناعي ذاتي يسبب ضعف العضلات. ينتج الجسم أجساماً مضادة تهاجم الوصلة بين العصب والعضلات.
العلامات والأعراض
الأعراض الأكثر شيوعًا للوهن العضلي الوبيل هي أعراض الوهن العضلي الوبيل في العين (50%) مثل تدلي الجفون (تدلي الجفون)، والرؤية المزدوجة (ازدواج الرؤية) وعدم وضوح الرؤية. يمكن أن يعمم المرض بما في ذلك أعراض مثل ضعف عضلات الوجه والأطراف. علاوة على ذلك، يمكن أن يعاني المرضى من صعوبات في المضغ والبلع والكلام. قد يؤدي ضعف الجهاز التنفسي إلى فشل تنفسي حاد.
تتأثر أعراض الوهن العضلي الوبيل سلباً بالتمارين الرياضية والحرارة والمرض والإجهاد. وعادةً ما تتفاقم الأعراض في المساء وتتحسن بعد الراحة.

الأسباب
وغالباً ما يرتبط الوهن العضلي الوبيل بأمراض أخرى مثل التهاب المفاصل الروماتويدي وتصلب الجلد والذئبة الحمامية الجهازية. 65% من مرضى الوهن العضلي الوبيل لديهم تضخم في الغدة الصعترية. 15٪ من المرضى المصابين بالوهن العضلي الوبيل يعانون من ورم الغدة الصعترية.
الإجراءات التشخيصية
يتم تشخيص الوهن العضلي الوبيل سريرياً من قبل طبيب أعصاب متخصص، مدعوماً باختبارات محددة بما في ذلك اختبارات مثبطات الكولينستريز، واختبار الكشف عن الأجسام المضادة، وتخطيط كهربية العضلات، والتصوير المقطعي المحوسب والتصوير بالرنين المغناطيسي للصدر، للكشف عن ورم الغدة الصعترية أو تضخم الغدة الصعترية.
العلاج
إن علاج الوهن العضلي الوبيل فعال ومعظم المرضى قادرون على عيش حياة طبيعية. وبناءً على النتائج السريرية، يمكن أن يشمل العلاج بعض الأدوية (مثبطات الكولينستريز، والعوامل المثبطة للمناعة، والغلوبولين المناعي الوريدي (IVIG)، وفصادة البلازما، واستئصال الغدة الصعترية، والعلاج الطبيعي وتغيير نمط الحياة.
فريق الخبراء لدينا
منذ أكثر من عشر سنوات تعتبر GNC العيادة الرائدة في مجال طب الأعصاب في الإمارات العربية المتحدة. جميع خبراء الوهن العضلي الوبيل لدينا حاصلون على شهادة البورد الألماني ولديهم خبرة مهنية لا تقل عن 25 عامًا. إذا كنت تبحث عن أكثر خبراء الوهن العضلي الوبيل الموثوق بهم، فأنت في المكان الصحيح.
Testimonials
``It was a great visit thanks! It really helped me.``
``Great service``
``God bless you guys wish you more of success``
``I'm impressed by the Professor and team professionalism``
``Being able to have blood tests and EEG done at the clinic itself was very helpful and convenient. This also allowed my doctor to have fast access to the test results.``
``I am thankful for the service.``
``Excellent doctor``
``The doctor is the best and everyone's very helpful``
As Seen On
الاكتئاب
المرض
الاكتئاب
الاكتئاب - اضطراب قديم قدم تاريخ البشرية. وقد سبق لأبقراط (460-377 قبل الميلاد) أن وصف الميلانخوليا، وهي حالة تشبه إلى حد كبير الاكتئاب الحالي.
يتأثر أكثر من 350 مليون شخص على مستوى العالم بالاكتئاب ويمكن أن يصيب أي شخص - من الشباب إلى كبار السن. ولكن ما الذي يعنيه بالضبط التأثر بالاكتئاب؟ وما هي الأعراض الشائعة؟ وما هي العلاجات المتاحة؟
التعريف
الاكتئاب هو مرض طبي خطير يسبب الشعور المستمر بالحزن و/أو فقدان الاهتمام. ويسمى أيضًا بالاكتئاب الجسيم أو الاضطراب الاكتئابي الجسيم أو الاكتئاب السريري ويؤثر على مشاعرك وطريقة تفكيرك وطريقة تصرفك. يمكن أن يؤدي الاكتئاب إلى مجموعة متنوعة من المشاكل العاطفية والجسدية، وقد يجعلك تشعر كما لو أن الحياة لا تستحق العيش وغالباً ما يتعارض مع القيام بأنشطتك اليومية العادية.
الأعراض
يمكن أن تشمل الأعراض الحزن والفراغ وفقدان الاهتمام أو المتعة بالأنشطة التي اعتدت الاستمتاع بها، وتغير في الوزن، وصعوبة في النوم أو الإفراط في النوم، وفقدان الطاقة، والقلق والاضطراب أو الأرق، وبطء التفكير أو الكلام أو حركات الجسم، والشعور بانعدام القيمة والتفكير في الموت أو الانتحار.
النماذج
هناك عدة أشكال للاكتئاب. يمكن التمييز بين الاضطراب الاكتئابي الرئيسي، والاضطراب الاكتئابي المستمر (عسر المزاج)، والاكتئاب الذهاني، واكتئاب ما بعد الولادة، والاضطراب العاطفي الموسمي (SAD).
- اضطراب الاكتئاب الشديد: يتميز هذا الشكل بمزاج اكتئابي يستمر لأكثر من أسبوعين ويعيق حياة المريض، بما في ذلك العمل والحياة الخاصة والعلاقات والصداقات. يمكن أن تحدث النوبة مرة واحدة فقط في حياة الشخص، ولكن في كثير من الأحيان، يمر الشخص بعدة نوبات.
- الاضطراب الاكتئابي المستمر (عسر المزاج): يستمر هذا الشكل لمدة عامين على الأقل وقد يعاني المريض من نوبات اكتئاب شديد إلى جانب فترات من الأعراض الأقل حدة. ويعتبر هذا الشكل من الاكتئاب المزمن.
- الاكتئاب الذهاني: يحدث هذا الشكل عندما يعاني المريض من اكتئاب شديد بالإضافة إلى شكل من أشكال الذهان، مثل وجود معتقدات خاطئة مزعجة أو انقطاع عن الواقع (أوهام)، أو سماع أو رؤية أشياء مزعجة لا يستطيع الآخرون سماعها أو رؤيتها (هلوسة).
- اكتئاب ما بعد الولادة: هذا الشكل تعاني منه العديد من النساء بعد الولادة عندما تكون التغيرات الهرمونية والجسدية والمسؤولية الجديدة لرعاية المولود الجديد مرهقة. وهو أكثر خطورة من "اكتئاب ما بعد الولادة".
- الاضطراب العاطفي الموسمي: يتميز هذا النوع بأعراض الاضطراب الاكتئابي الموسمي فقط خلال وقت محدد من السنة، وعادةً ما يكون في فصل الشتاء. ويبدو أن هذا مرتبط بأيام الشتاء الأقصر ونقص ضوء الشمس في أجزاء كثيرة من البلاد.
الاكتئاب هو أكثر من مجرد "كآبة" أو شعور بالإحباط لبضعة أيام. إنه مرض طبي وليس علامة ضعف.
الأسباب
هناك عدد من العوامل التي قد تزيد من فرصة الإصابة بالاكتئاب ولكن من غير المعروف بالضبط ما الذي يسبب هذا المرض. العوامل التي يمكن أن تكون متورطة في ذلك هي الاختلافات البيولوجية وكيمياء الدماغ والهرمونات والصفات الموروثة وأحداث الحياة. على الأرجح، يحدث الاكتئاب بسبب مزيج من هذه العوامل. من المفترض حسب نظريات طويلة الأمد حول الاكتئاب أن الناقلات العصبية المهمة - المواد الكيميائية التي تستخدمها خلايا الدماغ للتواصل - غير متوازنة. وقد أظهرت تقنيات تصوير الدماغ، مثل التصوير بالرنين المغناطيسي (MRI)، أن أدمغة الأشخاص المصابين بالاكتئاب تبدو مختلفة عن أدمغة الأشخاص غير المصابين بالاكتئاب. وتبدو أجزاء الدماغ المرتبطة بالمزاج والتفكير والنوم والشهية والسلوك مختلفة.
علاوة على ذلك، يمكن أن ينتج خطر الإصابة بالاكتئاب عن تأثير العديد من الجينات التي تعمل مع عوامل بيئية أو عوامل أخرى كما تشير الأبحاث. بالإضافة إلى ذلك، قد تؤدي الصدمة النفسية أو فقدان شخص عزيز أو علاقة صعبة أو أي موقف مجهد إلى حدوث نوبة اكتئاب. قد تحدث نوبات اكتئاب أخرى مع أو بدون محفز واضح.
العلاج
يجب أن يكون الفحص البدني الشامل من قبل الطبيب الخطوة الأولى للحصول على العلاج لاستبعاد الأسباب المحتملة الأخرى للأعراض. بعد ذلك يجب إجراء تقييم تشخيص للاكتئاب من قبل طبيب نفسي أو أخصائي صحة نفسية. يعتمد العلاج على نوع الاكتئاب الذي قد تعاني منه. على سبيل المثال، يتم علاج بعض المرضى الذين يعانون من الاكتئاب السريري بالعلاج النفسي والبعض الآخر يتم وصف مضادات الاكتئاب لهم. كما يتم علاج آخرين ممن لا يستجيبون لعلاجات الاكتئاب القياسية بتقنيات تحفيز الدماغ مثل العلاج بالصدمات الكهربائية (ECT)، والذي يُطلق عليه أيضًا العلاج بالصدمات الكهربائية، أو التحفيز المغناطيسي عبر الجمجمة (TMS)، أو تحفيز العصب المبهم (VNS).
ومع ذلك، يجب أن تدرك أن الاكتئاب لن يتم الشفاء منه في يوم واحد فقط أو بحبة واحدة فقط. التحلي بالصبر أمر مهم وقد يتطلب الأمر تجربة مضادات اكتئاب مختلفة للعثور على أكثرها فعالية بالنسبة لك. العلاج النفسي هو علاج فعال ولكنه قد لا يكفي وحده لعلاج الاكتئاب الحاد. ولكن يمكن أن يلعب دوراً مهماً عند استخدامه مع العلاجات الأخرى، بما في ذلك الأدوية.
إذا لم تكن قادراً على معرفة ما هي حالتك النفسية التي تعاني منها، يمكننا مساعدتك في ذلك من خلال مساعدة أفضل أطباء الأعصاب والأطباء النفسيين لدينا.© GNC, German Neuroscience Center Dubai (Neurology, Psychiatry, Psychology, Counseling, Dubai, UAE)
الرؤية المزدوجة
ما هي الرؤية المزدوجة؟
يرى المريض المصاب بالرؤية المزدوجة صورتين لجسم واحد إما بشكل دائم أو متقطع. تُعرف الرؤية المزدوجة أيضاً باسم ازدواج الرؤية. قد تكون الإزاحة أفقياً أو رأسياً أو قطرياً. يمكن أن يكون إدراك الصورتين متداخلاً أيضاً. يجب أخذ أعراض الرؤية المزدوجة على محمل الجد، لأن بعض الأسباب تحتاج إلى علاج طبي عاجل.
الأعراض
قد تتنوع أعراض الرؤية المزدوجة كما هو موضح أعلاه، ولكن اعتمادًا على السبب، قد تظهر أعراض أخرى مع الرؤية المزدوجة، مثل
- اختلال في إحدى العينين أو كلتيهما
- ألم مع حركة العين في إحدى العينين أو كلتيهما
- ألم حول العينين، مثل الصدغين أو الحاجبين
- الصداع
- الغثيان
- ضعف في العينين أو في أي مكان آخر
- الجفون المتدليةالأسباب
هناك العديد من الأسباب المحتملة لازدواج الرؤية. إذا كانت الرؤية المزدوجة طويلة الأمد أو إذا كانت الرؤية المزدوجة تتكرر باستمرار، فقد تشمل أسبابها ما يلي:
- مشاكل الأعصاب: التصلب المتعدد، متلازمة غيلان باريه، داء السكري
- مشاكل القرنية: الهربس النطاقي، جفاف القرنية
- مشاكل العدسة: إعتام عدسة العين
- مشاكل الدماغ: سكتة دماغية، تمدد الأوعية الدموية، صداع نصفي، ورم في الدماغ، إصابة في الرأس
- مشاكل العضلات: الوهن العضلي الوبيلنظرًا لأن أسباب الرؤية المزدوجة قد تكون مهددة للحياة، فمن المهم جدًا استشارة أخصائي إذا لم تتوقف الأعراض.
الأنواع
هناك ثلاثة أنواع من الرؤية المزدوجة: الرؤية المزدوجة بالعينين والرؤية المزدوجة الأحادية والرؤية المزدوجة الفسيولوجية. لا تعمل عيون المرضى الذين يعانون من الرؤية المزدوجة ثنائية العينين معًا بشكل صحيح وتختفي الرؤية المزدوجة إذا قام المريض بتغطية عين واحدة. تحدث الرؤية المزدوجة الأحادية عندما تستمر الرؤية المزدوجة عند تغطية العين غير المصابة. في الرؤية المزدوجة الفسيولوجية للرؤية المزدوجة الفسيولوجية تظهر الأجسام الخلفية التي لا يركز عليها المريض بشكل مضاعف. وغالباً ما تمر مشكلة الرؤية هذه دون أن يلاحظها أحد لأن دماغ المريض عادةً ما يستطيع تعويض هذا النوع من الرؤية المزدوجة.
العلاج
نظراً لأن العديد من الأمراض المختلفة يمكن أن تؤدي إلى ظهور أعراض الرؤية المزدوجة، فقد يكون من الصعب معرفة السبب الحقيقي. من المهم إجراء فحص شامل لتحديد سبب الرؤية المزدوجة. في الواقع، قد تكون الحالة مسألة حياة أو موت، مثل ورم في الدماغ أو تمدد الأوعية الدموية. بعض الحالات التي تسبب الرؤية المزدوجة يصعب وأحياناً يستحيل علاجها. تتسبب بعض السكتات الدماغية والشلل العصبي في الرؤية المزدوجة المتقلبة التي لا يمكن قياسها بدقة كافية لتصحيحها.
لتشخيص الرؤية المزدوجة ولمعرفة سبب هذه الأعراض، يستخدم طبيب الأعصاب طرقاً متعددة مثل اختبارات الدم والفحص العصبي الشامل وربما دراسات التصوير مثل التصوير المقطعي المحوسب والتصوير بالرنين المغناطيسي. يعتمد العلاج على النتائج. إذا كان ضعف عضلات العين هو سبب الرؤية المزدوجة فقد تساعد الجراحة. إذا كان الوهن العضلي الوبيل أو داء السكري هو السبب فإن الأدوية ستساعد.
القلق والرهاب ونوبات الهلع والرهاب ونوبات الهلع
المرض
القلق، الرهاب، نوبات الهلع، رهاب الخوف، الخوف من الأماكن المكشوفة، الخوف
هناك شيء واحد مشترك بين القلق والرهاب ونوبات الهلع ورهاب الخلاء. الخوف. الخوف هو شعور يعرفه الجميع على أنه شعور طبيعي تماماً. الخوف عادة ما يكون رد فعل لموقف مخيف مثل سرقة بنك أو أي موقف خطير آخر. يتحول الخوف الطبيعي إلى اضطرابات قلق أو رهاب عندما يحدث رد فعل خائف لا يتوافق مع الحدث الفعلي، أي موقف يصنفه غالبية الناس على أنه غير مخيف على الإطلاق، أو إذا كان رد فعل القلق قويًا بشكل غير طبيعي بحيث يكون لدى المريض انطباع بأنه سيتقيأ أو سيُغمى عليه أو يموت أو يصاب بالجنون.
التعريف والأعراض والعلامات
نوبات الهلع
نوبات الهلع هي نوبات خوف قصيرة غير متوقعة. يمكن أن تتراوح مدتها بين 10 و20 دقيقة. وغالباً ما يعاني المريض من خفقان أو قشعريرة أو قشعريرة أو احمرار ساخن أو تعرق أو ارتجاف أو ارتعاش أو ارتعاش أو غثيان أو دوار أو تنميل أو وخز. علاوة على ذلك، قد يعاني المريض من ضيق في التنفس وألم في الصدر. قد يؤدي ذلك إلى الخوف من الإصابة بنوبة قلبية والخوف من الاختناق والخوف من فقدان السيطرة والخوف من فقدان العقل والخوف من الإغماء والخوف من الموت. لا يستطيع المرضى تحديد ما يخشونه على وجه الخصوص. وبالتالي يشعرون بالقلق من إمكانية حدوثها مرة أخرى. يمكن أن تحدث نوبات الهلع كاضطراب هلع أو تكون عرضًا لحالات أخرى مثل الرهاب أو اضطراب ما بعد الصدمة.
رهاب الخلاء
يصف رهاب الخلاء الخوف من الخوف من الوقوع في فخ الخوف من الوقوع في فخ وعدم القدرة على الهروب من مواقف أو أماكن معينة أثناء التعرض لنوبة هلع. قد تكون هذه المواقف: الابتعاد عن المنزل أو السفر، أو التواجد في أماكن مزدحمة، أو الوقوف في طابور، أو التواجد على جسر. وبالتالي يحاول المرضى تجنب كل هذه المواقف إلى درجة تقييدهم في جميع أنشطة الحياة اليومية تقريبًا أو حتى البقاء في المنزل. تكون الأعراض أقل إزعاجاً في بعض الأحيان إذا كان المريض بصحبة صديق موثوق به أو أحد أفراد العائلة
اضطراب الهلع
نحن نتحدث عن اضطراب الهلع إذا كانت نوبات الهلع متكررة أو إذا كان المريض قلقًا باستمرار من أن نوبة هلع أخرى ستعقبها. نفصل بين اضطراب الهلع المصحوب برهاب الخلاء واضطراب الهلع بدون رهاب الخلاء.
الاضطرابات المصاحبة
الاكتئاب
غالبًا ما يصاب المرضى الذين يعانون من نوبات/اضطرابات الهلع الحادة أو طويلة الأمد بالاكتئاب. ويزيد الخطر 10 أضعاف عن متوسط السكان. وهذا يؤدي إلى زيادة معدل محاولة الانتحار بنسبة 20%
الكحول وإساءة استخدام المواد المخدرة
غالبًا ما يصاب المرضى الذين يعانون من نوبات/اضطرابات الهلع الحادة أو طويلة الأمد بالاعتماد على الكحول أو المواد الأخرى أو إساءة استخدامها. ويكون الخطر أعلى بمرتين من متوسط عدد السكان.
التشخيص
من المهم استبعاد أو استبعاد جميع الأسباب العضوية/الجسدية للأعراض التي تظهر مثل النوبة القلبية وما إلى ذلك. لذلك قد يكون من الضروري إجراء: الفحص البدني، وضغط الدم، والفحوصات المخبرية الشاملة، وتخطيط القلب، وتخطيط صدى القلب، وتخطيط الدماغ، والتصوير المقطعي المحوسب، والتصوير بالرنين المغناطيسي.
إذا كنت غير قادر على معرفة ما هي مشكلتك النفسية، يمكننا مساعدتك في ذلك من خلال مساعدة أفضل أطباء الأعصاب والأطباء النفسيين والأطباء النفسيين.العلاج
هناك طرق فعالة للغاية لعلاج نوبات الهلع / الاضطرابات المرتبطة بالخوف. أفضل الممارسات هي الجمع بين ما يلي:
العلاج النفسي
العلاج السلوكي المعرفي والعلاج بالتعرض هو الخيار الأول للعلاج وأظهر تحسنًا في 70-80% من المرضى.
الدواء
مضادات الاكتئاب هي الخيار الأول للأدوية المضادة للاكتئاب. أظهر ما يصل إلى 85% من المرضى تحسناً. الأدوية الأخرى قوية جداً على المدى القصير وتظهر انخفاضاً كبيراً في الأعراض والخوف.
تغييرات في نمط الحياة
تُعد برامج إدارة التوتر ومجموعات الدعم مساعدة كبيرة للمرضى الذين يعانون من اضطرابات الهلع.
© GNC, German Neuroscience Center Dubai (Neurology, Psychiatry, Psychology, Counseling, Dubai, UAE)
فقدان الذاكرة ومشاكل الذاكرة والنسيان
يمكن أن يكون فقدان الذاكرة ومشاكل الذاكرة مثل النسيان أمراً مقلقاً، مما يؤثر على مختلف جوانب الحياة اليومية. يُعد التقييم الطبي الفوري أمراً بالغ الأهمية عند مواجهة مشاكل الذاكرة. يلتزم المركز الألماني لطب الأعصاب، باعتباره مركزاً رائداً لطب الأعصاب في دبي، بتقديم معلومات شاملة حول مشاكل الذاكرة. في هذه المقالة، نتناول في هذه المقالة العلامات والأعراض وعوامل الخطر والأسباب والتشخيص والعلاج وغيرها من المعلومات ذات الصلة بالمرضى الذين يعانون من مشاكل الذاكرة.
فقدان الذاكرة: العلامات والأعراض
يمكن أن تظهر مشاكل الذاكرة بعدة طرق، بدرجات متفاوتة من الشدة. تشمل العلامات والأعراض الشائعة ما يلي:
- النسيان: النسيان المتكرر للأحداث أو المواعيد أو المحادثات الأخيرة.
- صعوبة التركيز: صعوبة التركيز على المهام أو اتخاذ القرارات أو متابعة المحادثات.
- الارتباك: الشعور بالارتباك أو الارتباك بشأن الزمان أو المكان أو الأشخاص.
- وضع الأغراض في غير مكانها: كثرة فقدان الأغراض أو وضعها في غير محلها في أماكن غير معتادة.
- الأسئلة المتكررة: طرح نفس الأسئلة بشكل متكرر خلال فترة زمنية قصيرة.
عوامل خطر الإصابة بمشكلات الذاكرة
تزيد بعض العوامل من احتمالية التعرض لمشاكل في الذاكرة، بما في ذلك:
- العمر: يعد التقدم في العمر عامل خطر شائع للتدهور المعرفي ومشاكل الذاكرة.
- الحالات الطبية: يمكن أن تساهم حالات مثل مرض الزهايمر والخرف الوعائي وضعف الإدراك المعتدل في حدوث مشاكل في الذاكرة.
- التاريخ العائلي: يمكن أن يزيد التاريخ العائلي للتدهور المعرفي أو الاضطرابات العصبية التنكسية من خطر الإصابة.
الأسباب الشائعة لمشاكل الذاكرة
يمكن أن تنبع مشاكل الذاكرة من أسباب كامنة مختلفة:
- الحالات العصبية: يمكن أن تؤثر الاضطرابات العصبية التنكسية مثل الزهايمر ومرض باركنسون على الذاكرة.
- الاكتئاب والقلق: يمكن أن تؤثر اضطرابات المزاج على الذاكرة والوظيفة الإدراكية.
- الأدوية: بعض الأدوية لها آثار جانبية إدراكية تؤثر على الذاكرة.
- اضطرابات النوم: يمكن أن يؤدي النوم غير الكافي أو اضطرابات النوم إلى إضعاف الوظيفة الإدراكية.
التشخيص والتقييم
يتطلب تشخيص مشاكل الذاكرة إجراء تقييم شامل، بما في ذلك:
- التاريخ الطبي: جمع المعلومات عن الحالات الطبية والأدوية والتاريخ العائلي.
- الاختبارات المعرفية: تقييم الذاكرة والانتباه ومهارات حل المشكلات من خلال اختبارات متخصصة. في المركز الألماني لعلم الأعصاب، نقدم في المركز الألماني لعلم الأعصاب أكثر الاختبارات النفسية العصبية تقدماً للكشف عن فقدان الذاكرة المبكر والضعف الإدراكي البسيط.
- التصوير: يمكن أن تكشف تقنيات التصوير الدماغي مثل التصوير بالرنين المغناطيسي والتصوير المقطعي بالإصدار البوزيتروني عن تشوهات هيكلية.
- تخطيط كهربية الدماغ (EEG): يقيس تخطيط كهربية الدماغ النشاط الكهربائي للدماغ من خلال تسجيل الإشارات التي تنتجها الخلايا العصبية باستخدام أقطاب كهربائية توضع على فروة الرأس. يتم عرض هذا النشاط على شكل أنماط موجية، والتي توفر نظرة ثاقبة لوظائف الدماغ والاضطرابات المحتملة. تخطيط كهربية الدماغ هو إجراء غير جراحي آمن وغير مؤلم، مما يجعله أداة قيّمة لتشخيص الخرف ومراقبته. وغالباً ما تُظهر الأنواع المختلفة من الخرف، مثل مرض الزهايمر والخرف الوعائي وخرف أجسام ليوي، أنماطاً محددة من تخطيط كهربية الدماغ. يمكن أن يساعد تخطيط كهربية الدماغ في التمييز بين هذه الأشكال المختلفة من الخرف بناءً على البصمات الكهربائية الفريدة المرتبطة بكل نوع.
- الفحوصات المخبرية: يمكن أن تحدد اختبارات الدم الحالات الطبية الكامنة التي تساهم في حدوث مشاكل في الذاكرة.
مناهج علاج النسيان وفقدان الذاكرة
يعتمد نهج علاج مشاكل الذاكرة على السبب الكامن وراءها وشدتها:
- تعديلات نمط الحياة: اعتماد نمط حياة صحي للدماغ مع ممارسة التمارين الرياضية بانتظام واتباع نظام غذائي متوازن والنوم الكافي.
- إعادة التأهيل المعرفي: الانخراط في التمارين الإدراكية لتحسين الذاكرة والوظائف الإدراكية.
- الأدوية: في بعض الحالات، يمكن أن تساعد الأدوية في بعض الحالات في السيطرة على الأعراض أو إبطاء تطور الحالات الكامنة. وقد حصلت بعض الأدوية الواعدة مؤخرًا على موافقة إدارة الغذاء والدواء الأمريكية ويمكن استخدامها حسب الحالة الفردية.
- العلاجات: يمكن أن تساعد العلاجات السلوكية والاستشارات ومجموعات الدعم في التعامل مع تحديات الذاكرة.
متى تزور الطبيب
يُعد التقييم الطبي الفوري أمراً بالغ الأهمية عند مواجهة مشاكل في الذاكرة:
- الأعراض المستمرة: إذا استمرت مشاكل الذاكرة أو تفاقمت مع مرور الوقت، استشر الطبيب.
- الاضطراب في الحياة اليومية: إذا كانت تحديات الذاكرة تعيق المهام اليومية أو العمل أو العلاقات اليومية، فاطلب العناية الطبية.
- التغيرات المفاجئة: يتطلب الظهور السريع لمشاكل الذاكرة أو التدهور المعرفي تقييمًا طبيًا فوريًا.
- مخاوف بشأن أحبائك: إذا لاحظت مشاكل في الذاكرة لدى أحد أفراد العائلة أو الأصدقاء، شجعهم على طلب المساعدة.
الخاتمة
يمكن أن يؤثر فقدان الذاكرة ومشاكل الذاكرة على الأفراد من جميع الأعمار، مما يؤثر على الأداء اليومي ونوعية الحياة. في المركز الألماني لعلم الأعصاب بدبي، نقدم في المركز الألماني لعلم الأعصاب بدبي رعاية متخصصة ودعمًا للأشخاص الذين يعانون من مشاكل الذاكرة. من خلال التعرف على العلامات وفهم عوامل الخطر والسعي إلى التقييم والعلاج في الوقت المناسب، يمكن للأفراد معالجة مشاكل الذاكرة بشكل استباقي وتعزيز صحتهم المعرفية. يلتزم فريقنا المتفاني من أطباء الأعصاب بتقديم رعاية مخصصة لمساعدة المرضى في رحلتهم نحو تحسين صحة الذاكرة. اتصل بنا لحجز موعدك الآن.
مرض ثنائى القطب
الاضطراب ثنائي القطب
الاضطراب ثنائي القطب، المعروف سابقًا باسم اضطراب الهوس الاكتئابي، هو مصطلح شائع الاستخدام بهدوء هذه الأيام. وقد أعلن العديد من المشاهير أنهم يعانون منه؛ مثل روبن ويليامز وميل جيبسون وكاثرين زيتا جونز وإيمي واينهاوس وسيناد أوكونور وبريتني سبيرز وجان كلود فان دام وأكسل روز وراسل براند وريتشارد دريفوس وغيرهم الكثير. علاوة على ذلك، يُعتقد أن العديد من الشخصيات التاريخية قد عانت من الاضطراب ثنائي القطب؛ مثل فرانك سيناترا وإرنست همنغواي وفنسنت فان جوخ وفريدريك نيتشه وفلورنس نايتنجيل وإدفارد مونش وإدغار آلان بو وغيرهم الكثير.
يبدو أن الاضطراب ثنائي القطب مرض شائع يعرفه الجميع بطريقة ما. ولكن ما هي الحقائق؟ في هذه المقالة نود أن نقدم لك لمحة عامة عن المرض ونجيب على السؤال الأكثر شيوعاً.
التعريف
كما يوحي الاسم، فإن الاضطراب ثنائي القطب هو اضطراب مزاجي حيث يمكن للمرضى أن يظهر عليهم كلا قطبي الحالة المزاجية بالتناوب. وهذا يعني أن المرضى يمكن أن يتحولوا بشكل متكرر من الهوس ("سعيد جداً") إلى الاكتئاب ("حزين جداً"). ولكن ما هو "السعيد جداً" أو الحزين "جداً"؟ من الذي يقرر ما إذا كان مزاجاً طبيعياً أم مرضاً؟ الإجابة واضحة. المعاناة نفسها هي التي تحدد المرض. بمعنى، يجب أن يكون السؤال الصحيح الذي يجب طرحه هو: هل هناك من يعاني؟ المريض نفسه أم المحيطين به؟ إذا لم يكن أحد يعاني فلا بأس مطلقًا أن يكون حزينًا أو سعيدًا في بعض الأحيان. إنه ينتمي إلى الحياة. لكن الوضع يتغير إذا كان هناك من يعاني من حزنه أو حتى وصل إلى حد الانتحار لأن المعاناة شديدة لدرجة أنه يبدو أنه لا يوجد مخرج. لهؤلاء الأشخاص الحق ويجب أن يحصلوا على المساعدة المهنية بسهولة. يجب ألا يكون هناك وصمة عار تعيقهم. هذا ليس ضعفًا أو فشلًا من أي نوع. وينطبق الأمر نفسه على المحيطين بهم. إذا كان هناك أشخاص آخرون يعانون من سلوك شخص آخر، فيجب أن تتاح لهم إمكانية التعبير عن معاناتهم والبحث عن المساعدة؛ على سبيل المثال زوجك "سعيد" لدرجة أنه يقامر بمدخراتك كلها لأنه يعتقد باستمرار أنه "محظوظ" في المرة القادمة. أو طيار "سعيد" ومفرط في الثقة بالنفس لدرجة أنه يعتقد أنه لم يعد بحاجة إلى النوم أو أي نوع من تدابير السلامة قبل أن يطير بك إلى وجهتك في العطلة. في هذه الحالات لن يعاني المريض نفسه ولكن هناك احتمال أن يعاني الآخرون.
ليس الطبيب النفسي أو أي طبيب آخر هو من يقرر في المقام الأول ما إذا كان شخص ما مريضًا عقليًا. بل المرضى أنفسهم والمحيطين بهم.
حقائق
على الرغم من أن العديد من الأشخاص الناجحين يعانون من الاضطرابات ثنائية القطب، إلا أنه مرض خطير. بعض الحقائق 11% إلى 15% من المرضى غير المعالجين ينتحرون. ما يصل إلى 50% يحاولون الانتحار. أكثر من 50% سيصابون بإساءة استخدام المخدرات أو الكحول. يزداد معدل الطلاق ثلاثة أضعاف. 50% سيصبحون عاطلين عن العمل بعد 6 أشهر من نوبة الهوس. 800 من أصل 100,000 شخص يعيشون في الولايات المتحدة يعانون منه. تكون البداية في الغالب بين 15-24 سنة. يتأثر كلا الجنسين بالتساوي. الاضطرابات ثنائية القطب أكثر شيوعًا في المناطق الحضرية وفي الطبقات الاجتماعية والاقتصادية العليا والأشخاص ذوي التعليم العالي.
الأسباب
لا تزال أسباب الاضطرابات ثنائية القطب غير معروفة. وعلى الأرجح لن يكون هناك سبب واحد بل أسباب متعددة العوامل. نموذج الإجهاد - الضعف - التأقلم هو نموذج شائع الاستخدام لتفسير الأمراض النفسية. يمكن للعلماء تحديد العديد من عوامل الخطر المختلفة؛ مثل التاريخ العائلي الإيجابي للاضطراب ثنائي القطب. فالمرضى الذين عانى والدهم أو والدتهم من الاضطراب ثنائي القطب لديهم خطر أعلى بنسبة 20% للإصابة به أيضًا. علاوة على ذلك، تم اكتشاف الولادة كعامل خطر. 45% من النساء اللاتي يعانين من الاضطراب ثنائي القطب عانين من أول نوبة في فترة ما بعد الولادة. يبدو أن الإجهاد - سواء كان جسديًا (مثل الأمراض الجسدية) أو نفسيًا (مثل العمل والعلاقات وما إلى ذلك) - يبدو أنه عامل خطر؛ وكذلك تعاطي المخدرات أو الكحول.
الأعراض والعلامات
الاكتئاب: يحدد التصنيف الدولي للأمراض ICD-10 3 أعراض رئيسية وهي المزاج المكتئب، وفقدان المتعة والاهتمام بالأنشطة، والإرهاق أو فقدان الطاقة. وقد تتمثل الأعراض الأخرى في نقص التركيز والذاكرة، واليأس، والشعور بالذنب وعدم الاستحقاق، والميول الانتحارية، واضطرابات النوم، وفقدان الشهية والوزن.
الهوس: يحدد التصنيف الدولي للأمراض (ICD-10) عرضين رئيسيين هما المزاج المبهج بشكل غير طبيعي أو المزاج المتهيج. يمكن أن تتمثل الأعراض الأخرى في قلة التركيز وتشتت الانتباه، وتسارع الأفكار، وسوء التقدير، والسلوك المتهور، وزيادة الاندفاع، وتضخم تقدير الذات، وزيادة الطاقة، وزيادة النشاط، وفرط النشاط، وسرعة الكلام، وانخفاض الحاجة إلى النوم، وزيادة الرغبة الجنسية، وفرط النشاط الجنسي.
الأعراض الذهانية: من الممكن أن تحدث أعراض ذهانية في كلتا النوبتين.
النماذج
يوصف الاضطراب ثنائي القطب الأول بأنه مزيج من نوبتين أو أكثر من الهوس والاكتئاب أو نوبات مختلطة.
يوصف الاضطراب ثنائي القطب الثاني بأنه مزيج من نوبتين أو أكثر من الهوس الخفيف والاكتئاب أو نوبات مختلطة.
يوصف الاضطراب ثنائي القطب سريع الدوران بأنه مزيج من 4 نوبات أو أكثر من الهوس والاكتئاب أو نوبات مختلطة في عام واحد.
يوصف الاضطراب ثنائي القطب ثنائي القطب سريع الدوران بأنه مزيج من 4 نوبات أو أكثر من الهوس والاكتئاب أو نوبات مختلطة في شهر واحد.
التشخيص
<pstyle="text-align: right;">كما هو الحال في أي مرض عقلي يجب أولاً استبعاد الأسباب العضوية الحادة. يجب أن يتم ذلك من قبل طبيب نفسي في دبي ويشمل الفحص البدني وفحوصات الدم والتصوير بالرنين المغناطيسي للدماغ يجب ألا يزيد عمره عن عام واحد. إذا كان يجب استخدام الأدوية فقد تكون هناك إجراءات تشخيصية أخرى قابلة للتطبيق مثل تخطيط كهربية الدماغ أو تخطيط القلب. في الخطوة الثانية يقوم الطبيب النفسي بإجراء الفحص النفسي وتقييم الأعراض بناءً على التصنيف الدولي للأمراض ICD-10 أو DSM-IV. وعلاوة على ذلك، هناك اختبارات نفسية عصبية متاحة لتقييم أعراض نوبات الهوس أو الاكتئاب تحت إشراف أفضل أطباء الأعصاب لدينا في دبي.
العلاج

هناك خيارات علاج فعالة للغاية للاضطرابات ثنائية القطب. الأولوية هي حماية المريض ومحيطه من أي نوع من المخاطر. سواء كان المريض نفسه من السلوكيات الخطرة أو الانتحار، أو كان محيطه من السلوكيات المتهورة أو سوء المعاملة. وبدون العلاج المناسب، فإن المرأة التي تعاني من الاضطراب ثنائي القطب ستفقد 9 سنوات من عمرها، و14 سنة من النشاط الفعال، و12 سنة من الصحة الطبيعية. ويرجع ذلك إلى حقيقة أن الاضطراب ثنائي القطب مرض مزمن. أكثر من 90% من الأشخاص الذين يعانون من نوبة هوس سيصابون بنوبة أخرى. كلما كانت البداية مبكرة، كلما كان التشخيص أسوأ. مع العلاج سيتحسن 90% من الأشخاص الذين يتلقون العلاج، و50% منهم سيتعافون من الأعراض.
ولكن قبل الخوض في التفاصيل، دعنا نلقي نظرة على أكبر العقبات التي تعترض طريق الوصول إلى هناك.
دافع العلاج. الخطوة الأكثر تعقيداً هي دائماً الخطوة الأولى. البحث عن المساعدة المهنية خطوة صعبة بالنسبة لمعظم الناس. يبدو أن وصمة المرض النفسي موجودة على نطاق واسع. وعلاوة على ذلك، فإن العلاج الداخلي الذي قد يكون ضروريًا لا سيما في نوبات الهوس غالبًا ما يكون غير كافٍ. حتى لو كان المحيط يعاني من سلوك المريض، فإن المريض في نوبات الهوس قد لا يكون على علم بذلك. ومن الصعب على مقدمي الرعاية إقناع المريض بأنه قد يكون هناك خطأ ما. وغالبًا ما يدرك المرضى عواقب سلوكهم فقط بعد انتهاء نوبة الهوس أو إذا كانت لها عواقب وخيمة مثل عقوبة السجن أو الأضرار الصحية. أثناء المعاناة من نوبة الاكتئاب غالبًا ما ينخفض الدافع إلى الحد الذي يجعل المرضى غير قادرين على البحث عن المساعدة بأنفسهم. وهذا يوضح أهمية مقدمي الرعاية في الاضطرابات ثنائية القطب.
العقبة التالية هي الحفاظ على العلاج الناجح. حتى لو اكتشف المريض أن العلاج ساعده، فمن الشائع أن يتوقف عن تناول الدواء في مرحلة ما. فثلث إلى نصف مرضى الاضطراب ثنائي القطب يتوقفون عن تناول الدواء على عكس النصيحة. نظرًا لأن الاضطراب ثنائي القطب متكرر بشكل كبير، فهناك خطر كبير من الانتكاس.
العلاج الدوائي
في الاضطراب ثنائي القطب يتم استخدام أنواع مختلفة من الأدوية. يكون العلاج دائماً فردياً ويعتمد على العديد من العوامل، مثل التأثيرات التي عانى منها المريض في الماضي والآثار الجانبية والنوبات الحالية وشدة الأعراض وما إلى ذلك. الأدوية الشائعة الاستخدام هي مثبتات المزاج ومضادات الاكتئاب ومضادات الاختلاج والبنزوديازيبينات. يمكن أن يكون متوسط فترة العلاج 12 شهراً في المرضى الذين يعانون من مخاطر منخفضة للانتكاس و5 سنوات إلى أجل غير مسمى في المرضى الذين يعانون من مخاطر عالية للانتكاس.
علم النفس
يجب أن يقترن الدواء دائمًا بنوع من الدعم النفسي. من المهم إقامة علاقة موثوقة مع أخصائي الرعاية الصحية ووضع خطة علاج واقعية. يمكن أن تشمل العلاج السلوكي المعرفي أو العلاج الأسري أو العلاج الجماعي.
التثقيف النفسي
لا سيما في حالة الاضطراب ثنائي القطب، فإن المعرفة بالمرض أمر ضروري. للمرضى ومقدمي الرعاية أيضًا. من المهم تحديد عوامل الخطر والمحفزات الفردية وتطوير استراتيجيات لتجنبها. علاوة على ذلك، يجب أن يتعلم المريض كيفية اكتشاف الأعراض المبكرة لنوبة أخرى.
نمط الحياة
الهدف هو القضاء على جميع عوامل الخطر الفردية التي يمكن أن تؤدي إلى الانتكاس. يمكن أن يشمل ذلك نمط النوم وتعاطي المخدرات والضغط في العمل أو في الأسرة. يمكن إثبات أن الانتكاسة أقل احتمالاً إذا تم الحفاظ على نمط نوم جيد.
مجموعات الدعم
من المهم الحصول على طبيب نفسي جيد ودعم صحي متخصص. ولكن، إلى جانب ذلك، من المفيد جداً الحصول على مساعدة من المصابين الآخرين أو مقدمي الرعاية أيضاً. هنا يمكنك العثور على مزيد من المعلومات حول مجموعة الدعم المجانية.
References
- Poolsup N, Li Wan Po A, de Oliveira IR. Systematic overview of treatment in acute mania. J Clin Pharm Ther. 2000;25:139-56
- Macritchie K, Geddes JR, Scott J, et al. V for acute mood episodes in bipolar disorder. Cochrane Database Syst Rev. 2003:CD4052
- Davis JM, Janicak PG, Hogan DM. M in the prevention of recurrent affective disorders: a meta-analysis. Acta Psychiatr Scand. 1999;100:406-17
- Donna Sudak, MD
- Tondo L, Hennen J, Baldessarini RJ. Lower suicide risk with long-term L treatment in major affective illness: a meta-analysis. Acta Psychiatr Scand. 2001;104:163-72
- Geddes JR, Burgess S, Hawton K, et al. Long-term L therapy for bipolar disorder: systematic review and meta-analysis of randomized controlled trials. Am J Psychiatry. 2004;161:217-22
- Goodwin GM, Bowden CL, Calabrese JR, et al. A pooled analysis of 2 placebo-controlled 18-month trials of L and L maintenance in bipolar I disorder. J Clin Psychiatry. 2004;65:432-41
- Macritchie KA, Geddes JR, Scott J, et al. V acid, V and D in the maintenance treatment of bipolar disorder. Cochrane Database Syst Rev. 2001:CD3196
- Ceron-Litvoc D, Soares BG, Geddes J, et al. Comparison of C and L in treatment of bipolar disorder: a systematic review of randomized controlled trials. Hum Psychopharmacol. 2009;24:19-28
- Rendell JM, Gijsman HJ, Keck P, et al. O alone or in combination for acute mania. Cochrane Database Syst Rev. 2003:CD4040
- Yatham LN, Grossman F, Augustyns I, et al. Mood stabilisers plus r or placebo in the treatment of acute mania: international double-blind, randomised controlled trials. [Erratum in Br J Psychiatry 2003;182:369] Br J Psychiatry. 2003;182:141-7
- Rendell JM, Gijsman HJ, Bauer MS, et al. R alone or in combination for acute mania. Cochrane Database Syst Rev. 2006:CD4043
- Lenox RH, Newhouse PA, Creelman WL, Whitaker TM. Adjunctive treatment of manic agitation with L versus H : a double-blind study. J Clin Psychiatry. 1992;53:47-52
- Meehan K, Zhang F, David S, et al. A double-blind, randomized comparison of the efficacy and safety of intramuscular injections of O , L or placebo in treating acutely agitated patients diagnosed with bipolar mania. J Clin Psychopharmacol. 2001;21:389-97
- Gijsman HJ, Geddes JR, Rendell JM, et al. A for bipolar depression: a systematic review of randomized controlled trials. Am J Psychiatry. 2004;161:1537-47
- Nolen WA, Bloemkolk D. Treatment of bipolar depression: a review of the literature and a suggestion for an algorithm. Neuropsychobiology. 2000;42:11-17
- Delbello MP, Schwiers ML, Rosenberg HL, Strakowski SM. A double-blind, randomized, placebo-controlled study of Q as adjunctive treatment for adolescent mania. J Am Acad Child Adolesc Psychiatry. 2002;41:1216-23
- Derry S, Moore RA. Atypical A in bipolar disorder: systematic review of randomised trials. BMC Psychiatry. 2007;7:40
- Geddes JR, Calabrese JF, Goodwin GM. L for treatment of bipolar depression: independent meta-analysis and meta-regression of individual patient data from five randomised trials. Brit J Psychiatry. 2009:194:4-9
- Scott J, Garland A, Moorhead S. A pilot study of cognitive therapy in bipolar disorders. Psychol Med. 2001;31:459-67
- Beynon S, Soares-Weiser K, Woolacott N, et al. Psychosocial interventions for the prevention of relapse in bipolar disorder: a systematic review of controlled trials. Brit J Psychiatry 2008;192:5-11
- Miklowitz DJ, George EL, Richards JA, et al. A randomized study of family-focused psychoeducation and pharmacotherapy in the outpatient management of bipolar disorder. Arch Gen Psychiatry. 2003;60:904-12
- Rea MM, Tompson MC, Miklowitz DJ, et al. Family-focused treatment versus individual treatment for bipolar disorder: results of a randomized clinical trial. J Consult Clin Psychol. 2003;71:482-92
- Colom F, Vieta E, Martinez-Aran A, et al. A randomized trial on the efficacy of group psychoeducation in the prophylaxis of recurrences in bipolar patients whose disease is in remission. Arch Gen Psychiatry 2003;60:402-7
- Perry A, Tarrier N, Morriss R, et al. Randomised controlled trial of efficacy of teaching patients with bipolar disorder to identify early symptoms of relapse and obtain treatment. BMJ 1999;318:749-63
اضطرابات الأكل
المرض
اضطرابات الأكل، الشره المرضي العصبي، فقدان الشهية العصبي، فقدان الشهية العصبي
ما هي اضطرابات الأكل؟
اضطرابات الأكل هي حالات تُعرف بعادات الأكل غير الطبيعية التي قد تنطوي إما على تناول كميات غير كافية أو مفرطة من الطعام على حساب الصحة البدنية والعقلية للفرد. الشره المرضي العصبي وفقدان الشهية العصبي واضطراب نهم الطعام هي أكثر أشكال اضطرابات الأكل شيوعاً.
يمكن أن تسبب اضطرابات الأكل مشاكل جسدية خطيرة وقد تكون مهددة للحياة. وغالباً ما تظهر خلال سنوات المراهقة أو سن البلوغ، ولكنها قد تظهر أيضاً خلال مرحلة الطفولة أو في وقت لاحق من الحياة.
الأنواع والأعراض
فقدان الشهية العصبي
يتسم فقدان الشهية العصبي بسلوك غير طبيعي في الأكل، وهوس بالطعام والنحافة، وأحيانًا إلى حد التجويع الذاتي المميت. يعاني الشخص المصاب بفقدان الشهية من خوف شديد من اكتساب الوزن، وصورة مشوهة للجسم، وتقدير للذات يتأثر بشدة بتصورات وزن الجسم وشكله، أو إنكار لخطورة انخفاض وزن الجسم. حتى لو كان المريض يعاني من نقص الوزن فإنه يرى نفسه زائد الوزن. علاوة على ذلك، يتسم المرض برفض الأكل وإنكار الجوع والإفراط في ممارسة الرياضة والخوف من تناول الطعام في الأماكن العامة.
يمكن أن تشمل العواقب الجسدية لفقدان الشهية العصبي ترقق العظام (هشاشة العظام أو هشاشة العظام)، وهشاشة الشعر والأظافر، وجفاف الجلد واصفراره، ونمو الشعر الناعم في جميع أنحاء الجسم (لانوغو)، وانخفاض ضغط الدم، وتباطؤ التنفس والنبض، وتلف بنية القلب ووظيفته، وتلف الدماغ، وفشل الأعضاء المتعددة، والعقم.
الشره المرض العصبي
يتميز الشره المرضي العصبي بنوبات من تناول كميات كبيرة من الطعام في مدة قصيرة يتبعها تقيؤ قسري أو الإفراط في استخدام الملينات أو مدرات البول أو الصيام أو الإفراط في ممارسة الرياضة أو مزيج من هذه السلوكيات. قد يكون الأشخاص المصابون بهذا المرض بوزن طبيعي أو حتى بوزن زائد قليلاً، على الرغم من أنهم غالبًا ما يخشون زيادة الوزن، ويرغبون بشدة في إنقاص وزنهم وهم غير راضين بشدة عن حجم أجسامهم وشكلها.
يمكن أن تشمل العواقب الجسدية للشره المرضي العصبي التهاب الحلق والتهاب مزمن والتهاب الحلق، وتورم الغدد اللعابية في منطقة الرقبة والفك، واضطراب في عمل الأمعاء، وتلف الأسنان واللثة، وعدم انتظام ضربات القلب، وعدم انتظام الدورة الشهرية أو انقطاعها واختلال توازن الكهارل الذي يمكن أن يؤدي إلى نوبة قلبية.
اضطراب نهم الطعام
يفقد الأشخاص المصابون باضطراب نهم الطعام السيطرة على تناول الطعام. فهم يأكلون كميات مفرطة من الطعام (نهم الطعام)، ولكن على عكس فقدان الشهية والشره المرضي لا يحاولون تعويض هذا السلوك بممارسة الرياضة أو الصيام أو التطهير. يتميز اضطراب نهم الأكل بتناول الطعام إلى حد الانزعاج أو الألم، وتناول الطعام بشكل أسرع، وتناول الطعام بشكل متكرر بمفرده.
ونتيجة لذلك، غالبًا ما يعاني الأشخاص المصابون باضطراب نهم الطعام من زيادة الوزن أو السمنة. وهم أكثر عرضة للإصابة بأمراض القلب والأوعية الدموية وارتفاع ضغط الدم. وعلاوة على ذلك، غالبًا ما يشعر الأشخاص المصابون بهذا المرض بالاكتئاب أو الاشمئزاز أو الانزعاج من الكمية التي يتناولونها. ويعانون من الشعور بالذنب والخجل والضيق بسبب نهمهم في تناول الطعام، مما قد يؤدي إلى مزيد من الشراهة في تناول الطعام.
الأسباب
تتعدد أسباب اضطرابات الأكل. تشمل الأسباب المحتملة الأسباب البيولوجية والصحة النفسية والعقلية والمجتمع. قد تكون هناك جينات تجعل بعض الأشخاص أكثر عرضة للإصابة باضطرابات الأكل. قد يعاني الأشخاص الذين يعانون من هذه الاضطرابات من مشاكل نفسية وعاطفية مثل تدني احترام الذات التي تساهم في حدوث الاضطراب. علاوة على ذلك، غالبًا ما يزرع المجتمع الرغبة في النحافة، خاصة في الثقافة الغربية الحديثة.
العلاج
العلاج النفسي والتثقيف الغذائي والأدوية هي طرق علاج فعالة لاضطرابات الأكل. ويساعد العلاج النفسي الفردي أو الجماعي أو العائلي المريض على تعلم كيفية استبدال العادات غير الصحية بأخرى صحية. ينصب التركيز الرئيسي للعلاج على استعادة الشخص لوزنه الصحي، وعلاج المشاكل النفسية المتعلقة باضطراب الأكل وتقليل أو التخلص من السلوكيات أو الأفكار التي تؤدي إلى الأكل غير الصحي ومنع الانتكاس. يشيع استخدام العلاج السلوكي المعرفي في علاج اضطرابات الأكل، خاصةً في علاج الشره المرضي العصبي واضطراب نهم الطعام.
لا يمكن علاج اضطرابات الأكل عن طريق الأدوية، لكنها قد تساعد في السيطرة على الرغبة في الشراهة أو التطهير أو التحكم في الانشغالات المفرطة بالطعام والنظام الغذائي. نظرًا لأن اضطرابات الأكل غالبًا ما تحدث مع أدوية الاكتئاب والقلق مثل مضادات الاكتئاب ومضادات القلق ومثبتات المزاج قد تساعد أيضًا في علاج هذه الأعراض.
© GNC, German Neuroscience Center Dubai (Neurology, Psychiatry, Psychology, Counseling, Dubai, UAE)
انفصام الشخصية
ما هو الفصام؟
الفصام هو اضطراب دماغي. يؤثر على طريقة تصرف الشخص وتفكيره ورؤيته للعالم. وغالباً ما يكون لدى الأشخاص المصابين بالفصام إدراك مختلف للواقع بل ويفقدون الاتصال بالواقع. قد يرون أشياءً لا يراها الآخرون أو قد يسمعون أصواتًا لا يسمعها الآخرون (هلوسة). حتى أنهم قد يتحدثون بطريقة مشوشة أو قد يؤمنون بـ "واقعهم" الخاص (الوهم). حتى أن بعض الأشخاص يشعرون بالاضطهاد أو المراقبة المستمرة (جنون العظمة). ويعاني آخرون من سلوك غير منظم أو ما يسمى بـ "الأعراض السلبية"، مثل قلة التعبيرات العاطفية أو قلة الحماس. إذا ظهرت على الشخص أعراض كتغير جذري في الشخصية وضعف في الأداء بالإضافة إلى إحساس مشوه أو غير موجود بالواقع، فإننا نتحدث في المصطلحات الطبية عن "الذهان".
يبدأ الفصام عادةً في بداية مرحلة البلوغ، بين سن 15 و25 عامًا. تميل النساء إلى الإصابة بالأعراض الأولى بعد عدة سنوات من الرجال، وعادةً ما يكون ذلك في سن 25 عامًا تقريبًا. ومع ذلك، يتأثر الرجال أكثر من النساء. قد تتطور الأعراض ببطء أو في بعض الأحيان تظهر المتلازمة الكاملة على الفور. قد تكون علامات التحذير المبكرة للفصام هي الانسحاب الاجتماعي أو الاكتئاب أو الشك أو الضحك أو البكاء غير اللائق. من المهم أن تكون على دراية بالأعراض المبكرة، لأنه كلما تم تشخيص الاضطراب في وقت مبكر كلما كان من الأفضل علاجه.
يصيب الفصام ما يقرب من 0.7 إلى 1.0 في المئة من السكان البالغين في جميع أنحاء العالم. ويصاب حوالي 26 مليون شخص في جميع أنحاء العالم بالفصام. لذلك نقدر أن هناك حوالي 50 ألف شخص يعانون من الفصام في الإمارات العربية المتحدة.
في حين أن الفصام من بين الاضطرابات النفسية الشائعة، فإن اضطرابات القلق والمزاج مثل الاكتئاب أكثر شيوعًا من 5 إلى 10 أضعاف. في السنوات الماضية كان هناك رأي سائد منذ فترة طويلة مفاده أن معدل انتشار الفصام يختلف قليلاً من مجتمع إلى آخر. أما اليوم فلدينا مؤشرات تدل على أن معدلات الإصابة بالفصام يمكن أن تختلف باختلاف المناطق بسبب تأثير العوامل الثقافية والحضرية والجغرافية. فعلى سبيل المثال، ترتفع معدلات انتشار الفصام بين المهاجرين عن الأفراد المولودين في البلدان الأصلية وترتفع معدلات انتشاره في البلدان المتقدمة عن البلدان غير المتقدمة. وتوجد أعلى نسبة انتشار بين الأشخاص ذوي الوضع الاجتماعي والاقتصادي المنخفض الذين يعيشون في الدول النامية. تشير الدراسات الحديثة إلى أن العوامل البيئية المتعلقة بالإقامة في المناطق الحضرية قد تساهم في تطور الفصام.
نشرت منظمة الصحة العالمية بيانات عام 2002 بشأن انتشار مرض الفصام ونحن نعلم أن هذا الاضطراب يميل إلى أن يكون الأعلى في أوقيانوسيا والشرق الأوسط وآسيا مقارنة بأستراليا واليابان وأوروبا.
الأعراض والعلامات

هناك نوعان من الأعراض - الأعراض المبكرة التي قد توجد قبل سنوات من الظهور الفعلي لمرض الفصام، والأعراض الرئيسية. تشمل الأعراض المبكرة تغير الخبرة والوضوح في السلوك وإن كان بدرجة بسيطة بحيث لا يمكن ربطها بسهولة بالعلامات المبكرة للفصام.
الأعراض الرئيسية لمرض الفصام هي الضلالات، والهلوسة، والكلام غير المنظم، والسلوك غير المنظم، والأعراض السلبية مثل تضاؤل التعبير العاطفي أو التبلد. وتمثل هذه الأعراض المرحلة النشطة من الاضطراب والتي تظهر بعد التعرض لضغوطات أو تعاطي المخدرات أو بدون أي ضغوطات محددة. غالبًا ما يعاني المرضى من اضطرابات اجتماعية بسبب فقدان القدرات الشخصية مثل المبادرة والاهتمام والمتعة بالحياة والأشخاص الآخرين. قد تكون عواطفهم ضعيفة وقد يكون هناك فقر في الكلام وتراجع في النشاط والعناية الذاتية. علاوة على ذلك، غالباً ما يؤثر الفصام على المجالات المعرفية مثل الذاكرة والانتباه. كما أن نقص القدرة على اتخاذ القرار أمر شائع، خاصةً لدى المرضى الأكبر سناً.
الأسباب
اليوم أسباب الفصام غير معروفة تمامًا. يبدو أنه نتيجة تفاعل معقد بين العوامل الوراثية (الوراثية) والعوامل البيئية. يحتوي الفصام على عنصر وراثي قوي، مما يعني أن الأفراد الذين لديهم قريب من الدرجة الأولى مصاب بالفصام لديهم فرصة بنسبة 10% للإصابة بالاضطراب، أي أن نسبة الخطر أعلى بحوالي 15 مرة من متوسط السكان.
ولكن من المهم أن نذكر أن هذا الاضطراب يتأثر فقط بالعوامل الوراثية ولا تحدده الجينات. لذلك نحن نعلم أن الجينات الوراثية تجعل الشخص عرضة للإصابة بالفصام، ولكن العوامل البيئية تعمل على قابلية الإصابة بالفصام وتؤدي إلى ظهور الاضطراب. من الأبحاث التي نعرفها، أن العوامل "المحفزة للتوتر" قد تكون متورطة في الإصابة بالفصام، مثل الولادة لفترات طويلة، أو سوء التغذية قبل الولادة أو التعرض لعدوى فيروسية قبل الولادة. قد تساهم أيضًا مشاكل في بعض المواد الكيميائية التي تحدث بشكل طبيعي في الدماغ، بما في ذلك الناقلات العصبية التي تسمى الدوبامين والغلوتامات، في الإصابة بالفصام. تُظهر دراسات التصوير العصبي اختلافات في بنية الدماغ والجهاز العصبي المركزي للأشخاص المصابين بالفصام.
وصمة العار
في العديد من الثقافات تعتبر الصحة النفسية موضوعًا لا تتم مناقشته علنًا بل ويتم وصمه بالعار. سنساعد العديد من المرضى عندما نتمكن من التغلب على كوننا "صامتين" وندعمهم لطلب المساعدة المهنية. ستكون هذه الخطوة الأولى للحصول على العلاج وتحسين نوعية حياة المرضى وعائلاتهم. من العوائق التي تواجه العديد من المرضى الذين يعانون من أعراض مبكرة أيضًا أن الاضطرابات النفسية غالبًا ما تكون تغطيتها من قبل التأمين الصحي ضعيفة مما يؤدي إلى مزيد من التأخير في التشخيص والعلاج.
التشخيص
الفصام هو تشخيص سريري. سيتم طلب إجراء اختبارات معينة لاستبعاد الأمراض والحالات الأخرى التي قد تؤدي إلى ظهور أعراض شبيهة بالفصام. قد تشمل الاختبارات تعداد الدم الكامل، وتحليل البول، وتحليل البول، وملف التمثيل الغذائي، ودراسات التصوير والتقييم النفسي. سيقوم أفضل أخصائي نفسي في دبي بتقييم الحالة العقلية للمريض من خلال السؤال عن الأفكار والحالات المزاجية والهلوسة والسمات الانتحارية والميول العنيفة أو احتمالية العنف، بالإضافة إلى مراقبة سلوكه ومظهره. يجب إحالة المرضى الذين يُشتبه في إصابتهم بالفصام إلى التقييم النفسي. يجب أن يكون أحد الأعراض على الأقل الأوهام أو الهلوسة أو الكلام غير المنظم.
إذا كنت غير قادر على معرفة ما هي مشكلتك النفسية، فيمكننا مساعدتك في ذلك باستخدام أفضل أطباء الأعصاب في دبي والأطباء النفسيين في دبي والأخصائيين النفسيين في دبي.
علاج الفصام
يمكن علاج الفصام ويمكن علاج الفصام وتستمر النظرة المستقبلية للاضطراب في التحسن. ومع ذلك، فإن 50% فقط من المرضى يتلقون المساعدة الكافية. في كثير من الأحيان يمكن للأشخاص الذين يتلقون العلاج المناسب والمستمر أن يعيشوا حياة طبيعية ويعملوا. يجب علاج هذا الاضطراب في إطار معقد يشمل الأدوية والعلاج النفسي وإنشاء شبكة دعم قوية. لسوء الحظ، لا يتلقى العديد من المرضى العلاج المناسب اليوم بسبب عدم تقبل المجتمع و/أو عدم القدرة على الاعتراف بالحاجة إلى العلاج من قبل المرضى أنفسهم.
يتطلب العلاج الفعال مزيجًا من الأدوية والعلاج النفسي. يساعد العلاج في تخفيف العديد من أعراض الفصام، لكن معظم المصابين بهذا الاضطراب يتغلبون على الأعراض طوال حياتهم، وسيظل معظمهم يتناولون مضادات الذهان لبقية حياتهم. ومع ذلك، لا ينبغي استخدام مضادات الذهان كطريقة علاجية واحدة. يجب أن يستمر العلاج والتدخلات النفسية والاجتماعية.
تساعد العلاجات النفسية الاجتماعية المرضى على التعامل مع التحديات اليومية للمرض. يتيح تعلم واستخدام آليات التأقلم لمعالجة هذه المشاكل للأشخاص المصابين بالفصام الاختلاط الاجتماعي والالتحاق بالمدرسة والعمل. يمكن أن تكون مجموعات الدعم مساعداً فعالاً للأدوية أيضاً وتساعد المرضى على التواصل مع الآخرين الذين يواجهون تحديات مماثلة. قد تساعد مجموعات الدعم أيضًا الأسرة والأصدقاء على التأقلم.
ومع ذلك، يمكن للعديد من المصابين بالفصام أن يعيشوا حياة مجزية وذات مغزى.
© GNC, German Neuroscience Center Dubai (Neurology, Psychiatry, Psychology, Counseling, Dubai, UAE)
اضطراب ما بعد الصدمة – اضطراب ما بعد الصدمة
المرض
اضطراب ما بعد الصدمة أعراض اضطراب ما بعد الصدمة والعلاج والمزيد من أعراض اضطراب ما بعد الصدمة
.
ما هو اضطراب ما بعد الصدمة (PTSD)؟
اضطراب ما بعد الصدمة - اضطراب ما بعد الصدمة - هو حالة صحية عقلية خطيرة تحدث بعد حدث صادم. اضطراب ما بعد الصدمة هو نتيجة دائمة للمحن المؤلمة التي تسبب الخوف الشديد أو العجز أو الرعب. وقد يستمر لشهر أو حتى سنوات. وقد يبدأ مباشرة بعد الحدث أو يتأخر لأشهر. بعد تجربة أو مشاهدة حدث مرعب قد يواجه الشخص صعوبات في التأقلم والتكيف معه. قد يشعر الشخص بالتوتر أو الخوف حتى عندما لا يكون في خطر. وتستمر هذه المشاعر بل وتزداد، وتصبح قوية لدرجة أنها تمنع الشخص من عيش حياة طبيعية.
الأعراض
يمكن أن يشمل اضطراب ما بعد الصدمة (PTSD) العديد من الأعراض. وغالباً ما تبدأ في غضون ثلاثة أشهر من الحدث الصادم. هناك ثلاث فئات رئيسية لأعراض اضطراب ما بعد الصدمة:
- الاسترجاع: يسترجع الشخص المصاب باضطراب ما بعد الصدمة مرارًا وتكرارًا الحدث المؤلم كما لو كان يحدث مرة أخرى. قد يشمل ذلك ذكريات الماضي والكوابيس والهلوسة. كما قد يشعر الشخص المصاب باضطراب ما بعد الصدمة باضطراب عاطفي شديد أو ردود فعل جسدية تجاه شيء يذكره بالحدث.
- التجنب: يتجنب الشخص التفكير أو الحديث عن الحدث المؤلم. كما قد يتجنب أيضاً الأماكن أو الأحداث أو الأشياء التي تذكره بالصدمة النفسية مما قد يؤدي إلى الشعور بالانفصال والعزلة. قد يحدث شعور قوي بالذنب والاكتئاب.
- زيادة الاستثارة: قد يشعر الشخص بالتوتر والخوف وسهولة الفزع. وقد يعاني من مشاكل في النوم والتركيز بالإضافة إلى التهيج أو نوبات الغضب. قد تحدث أيضًا أعراض جسدية مثل زيادة ضغط الدم ومعدل ضربات القلب وسرعة التنفس وتوتر العضلات والغثيان والإسهال.
كما يمكن أن يشعر الشخص بالاكتئاب أو التخدير العاطفي. وأحياناً يحجب المريض الحدث تماماً من ذاكرته.
الأسباب
يمكن للشخص الذي يعاني من اضطراب ما بعد الصدمة أن يصاب باضطراب ما بعد الصدمة عندما يمر أو يشهد حدثاً صادماً مثل الانتهاك الجنسي أو التعذيب أو إساءة معاملة الأطفال أو حوادث السيارات أو الموت المفاجئ لأحد الأحباء أو كارثة طبيعية. يمكن أن يحدث اضطراب ما بعد الصدمة لدى أي شخص تعرض لحدث صادم، ولكن يُفترض أن يكون سببه مزيج من تنظيم الدماغ للمواد الكيميائية والهرمونات المسببة للتوتر والمخاطر الصحية العقلية الموروثة، مثل زيادة خطر الإصابة بالقلق والاكتئاب. وعلاوة على ذلك، تلعب التجارب الحياتية والجوانب الموروثة في الشخصية دوراً كبيراً.
إذا كنت غير قادر على معرفة ما هي مشكلتك النفسية، فيمكننا مساعدتك في ذلك بمساعدة أفضل أطباء الأعصاب والطب النفسي وأطباء علم النفس.
العلاج
علاج اضطراب ما بعد الصدمة فعال للغاية. الهدف منه هو دعم مهارات التأقلم لدى المريض ليكون قادرًا على التعامل مع الحدث المؤلم. تتمثل العلاجات الرئيسية للأشخاص المصابين باضطراب ما بعد الصدمة في العلاج النفسي أو الأدوية، وأحياناً كلاهما معاً. سيتعلم المريض مهارات معينة لمعالجة الأعراض وبالتالي تحسين الأعراض. يساعد الأخصائي النفسي في التأقلم في حالة ظهور أي أعراض مرة أخرى.
العلاج السلوكي المعرفي (CBT) هو علاج مفيد للغاية عند المعاناة من اضطراب ما بعد الصدمة. هناك عدة أجزاء للعلاج السلوكي المعرفي، بما في ذلك:
- العلاج بالتعرض: يساعد على مواجهة الخوف والسيطرة عليه عن طريق التخيل الذهني أو الكتابة أو زيارة المكان الذي وقع فيه الحدث.
- إعادة الهيكلة المعرفية: تساعد في التعرف على طريقة التفكير مثل الطرق السلبية أو غير الدقيقة في إدراك المواقف العادية. في بعض الأحيان يتذكر الناس الحدث بشكل مختلف عن كيفية حدوثه. يساعد الأخصائي النفسي على النظر إلى الأمور بطريقة واقعية.
- تدريب التلقيح ضد الإجهاد: يساعد في تقليل الأعراض عن طريق تقليل القلق. يساعد على النظر إلى الذكريات بطريقة صحية وواقعية.
كل هذه الأساليب يمكن أن تساعد في الحد من الخوف بعد حدث صادم. يجب مناقشة أفضل أنواع العلاج بشكل فردي مع الطبيب النفسي. علاوة على ذلك، يمكن لبعض الأدوية، مثل مضادات الاكتئاب والأدوية المضادة للقلق، أن تحسن من الشعور بالقلق والتوتر. يوصي الأخصائي أحياناً بمزيج من العلاج النفسي والأدوية.
وعلاوة على ذلك، سيتعلم مريض اضطراب ما بعد الصدمة تقنيات الاسترخاء مثل تدريب الاسترخاء الذاتي أو التدريب الذاتي. يوصى بأن يزور المريض مجموعة دعم أيضاً ليتعلم من المصابين الآخرين كيفية التعامل مع الموقف.
© GNC, German Neuroscience Center Dubai (Neurology, Psychiatry, Psychology, Counseling, Dubai, UAE)
التفاعل الحاد مع الإجهاد
Disease
اضطرابات الإجهاد في دبي: فهم وإدارة ردود الفعل الناتجة عن الإجهاد الحاد
هل تشعر بالإرهاق أو عدم القدرة على التأقلم مع أحداث الحياة اليومية أو تعاني من ضيق مستمر بعد حادث مؤلم؟ قد تكون تعاني من اضطراب التوتر الحاد. في المركز الألماني لعلم الأعصاب، نحن متخصصون في تقديم المساعدة والدعم المهني للأفراد الذين يعانون من اضطرابات التوتر في دبي. فريق الخبراء المتخصصين لدينا موجود هنا لإرشادك نحو حياة أكثر صحة وتوازناً.
يمكن أن تنشأ اضطرابات التوتر الحاد من أحداث الحياة الشديدة التي تعطل إحساسنا بالاستقرار والأمان. قد تشمل هذه الأحداث فقدان شخص عزيز أو تجارب العنف أو الانفصال أو الحوادث أو الصدمات أو سوء المعاملة. في بعض الأحيان، حتى الأحداث التي تبدو بسيطة مثل الذهاب إلى المدرسة أو الانتقال إلى مكان آخر يمكن أن تؤدي إلى رد فعل توتر. ومن الطبيعي الشعور بالحزن أو الصدمة أو الارتباك عند مواجهة مثل هذه الأحداث.
ومع ذلك، إذا استمر رد فعلك لفترة طويلة، أو أصبح لا يمكن السيطرة عليه، أو بدا غير متناسب مع الحدث نفسه، فإن طلب المساعدة المتخصصة أمر بالغ الأهمية. يمكن أن يظهر تأثير اضطرابات التوتر بطرق مختلفة، مثل تقييد الوعي، وانخفاض الانتباه، والارتباك، وفقدان الذاكرة، والاكتئاب، واليأس، والقلق، والعدوانية، وحتى الأعراض الجسدية مثل التعرق، وسرعة ضربات القلب، والاحمرار خجلاً.
عندما يحدث رد الفعل الحاد للتوتر مباشرةً بعد وقوع حدث ما ثم ينحسر تدريجيًا، فإنه يعتبر استجابة طبيعية. ومع ذلك، وبناءً على شدة الأعراض، قد يكون من الضروري طلب المساعدة المهنية لفترة قصيرة لاستعادة السيطرة على حياتك.
نتفهم في المركز الألماني لعلم الأعصاب التحديات الفريدة التي يواجهها الأفراد في دبي. يتخصص فريقنا من المتخصصين ذوي الخبرة في علاج اضطرابات الإجهاد، ويقدمون تقييمات شاملة وخطط علاجية مصممة خصيصاً لتلبية احتياجاتك الخاصة. نستخدم مناهج علاجية قائمة على الأدلة لمساعدتك على تطوير آليات فعالة للتكيف واستعادة الصحة النفسية واستعادة التوازن في حياتك.
توفر عيادتنا بيئة ترحيبية وداعمة حيث يمكنك مناقشة تجاربك ومخاوفك بصراحة. نحن نعطي الأولوية لصحتك النفسية ونلتزم بتوجيهك نحو مستقبل أكثر إشراقاً وصحة. يستخدم فريقنا نهجاً شاملاً يجمع بين العلاج والاستشارة والتدخلات الأخرى المثبتة لمعالجة الأسباب الجذرية لاضطرابات التوتر لديك.
عندما تختار المركز الألماني لعلم الأعصاب، فإنك تختار شريكاً موثوقاً به مكرساً لرفاهيتك. إن المعالجين الخبراء لدينا مزودون بالمعرفة والخبرة اللازمة للتغلب على تعقيدات اضطرابات التوتر، مما يوفر لك الأدوات اللازمة للتغلب على التحديات واستعادة السيطرة على حياتك.
لا تدع اضطرابات التوتر تعيق سعادتك وجودة حياتك. اتخذ الخطوة الأولى نحو الشفاء من خلال طلب المساعدة المتخصصة في المركز الألماني لعلم الأعصاب. اتصل بنا اليوم لحجز موعد والبدء في رحلتك نحو حياة خالية من التوتر ومُرضية.
تذكر، ليس عليك مواجهة اضطرابات التوتر بمفردك. في المركز الألماني لعلم الأعصاب، نحن هنا من أجلك في كل خطوة على الطريق.
احجز موعدك اليوم وابدأ رحلتك نحو صحة وسعادة أكبر. دعنا نكون شريكك في التغلب على اضطرابات التوتر في دبي.
إساءة المعاملة
سوء المعاملة مشكلة مقلقة للغاية تؤثر على الأفراد جسديًا وعاطفيًا ونفسيًا. يُعد التعرف على العلامات وفهم عوامل الخطر والبحث عن علاج فعال خطوات حيوية نحو التحرر من قبضته. يقف المركز الألماني لعلم الأعصاب في دبي كمنارة للأمل، حيث يقدم رعاية متخصصة ونهجاً متعدد التخصصات لمساعدة الضحايا على التغلب على سوء المعاملة واستعادة حياتهم.
علامات وأعراض سوء المعاملة
يمكن أن يظهر الإيذاء بأشكال مختلفة، تاركًا علامات وأعراضًا مميزة في أعقابه. قد يعاني الضحايا من إصابات غير مبررة، وغياب متكرر عن العمل أو الارتباطات الاجتماعية، وتغيرات مفاجئة في السلوك، والقلق، والاكتئاب، والانسحاب، وانخفاض احترام الذات. في المركز الألماني لعلم الأعصاب في دبي، يتم تدريب خبرائنا على التعرف على هذه العلامات وتقديم الدعم التعاطفي.
عوامل خطر إساءة المعاملة
يمكن أن تزيد بعض العوامل من احتمالية التعرض للإساءة. وتشمل هذه العوامل تاريخ الصدمة، وتدني احترام الذات، والافتقار إلى الدعم الاجتماعي، وتعاطي المخدرات، والاعتماد على الشخص الذي يسيء معاملتهم. يُعد التعرف على عوامل الخطر هذه أمراً ضرورياً للتدخل المبكر. يتمتع فريق المركز الألماني لعلم الأعصاب بالخبرة في تصميم التدخلات لمعالجة عوامل الخطر الفردية.
أسباب إساءة المعاملة
يمكن أن تنبع إساءة المعاملة من مجموعة متنوعة من الأسباب الكامنة، بما في ذلك ديناميكيات السلطة والصدمات النفسية التي لم يتم حلها ومشاكل الصحة العقلية والسلوكيات المكتسبة. إن فهم هذه الأسباب الجذرية أمر بالغ الأهمية لوضع خطط علاجية فعالة. يتعمق أطباؤنا في المركز الألماني لعلم الأعصاب بدبي في تاريخ الفرد لتحديد هذه الأسباب ووضع استراتيجيات علاجية مخصصة.
أشكال إساءة المعاملة
يتخذ الإيذاء أشكالاً مختلفة، ولكل منها تأثيره المدمر. ويشمل ذلك الإيذاء الجسدي والإيذاء العاطفي والنفسي والإيذاء الجنسي والإيذاء المالي والإهمال. قد يعاني الضحايا من مزيج من هذه الأشكال، مما يؤدي إلى ضائقة نفسية معقدة. يقدم المركز الألماني لعلم الأعصاب بدبي نهجاً شاملاً يعالج الآثار متعددة الأبعاد للإساءة.
التشخيص
التشخيص الدقيق هو حجر الزاوية في العلاج الفعال. يستخدم أخصائيونا في المركز الألماني لعلوم الأعصاب بدبي مجموعة من أدوات التشخيص، بما في ذلك التقييمات النفسية الشاملة والمقابلات والفحوصات الطبية. توفر هذه التقييمات رؤية شاملة للصحة البدنية والنفسية للفرد، مما يوجه عملية وضع خطة علاجية مصممة خصيصاً.
علاجات إساءة المعاملة
يتطلب التعافي من سوء المعاملة نهجاً متعدد الأوجه يدمج بين التدخلات الطبية والنفسية والدعم. يتعاون فريق الخبراء في المركز الألماني لعلم الأعصاب بدبي لوضع خطط علاجية مخصصة قد تشمل العلاج النفسي والاستشارة والأدوية ومجموعات الدعم والعلاجات الشاملة. يضمن التزامنا بالشفاء الشامل معالجة كل جانب من جوانب رفاهية المريض.
الطرائق العلاجية
في المركز الألماني لعلم الأعصاب بدبي، يتم استخدام مجموعة من الأساليب العلاجية القائمة على الأدلة لتسهيل الشفاء. العلاج المعرفي السلوكي المعرفي (CBT)، والعلاج الذي يركز على الصدمات، والعلاج السلوكي الجدلي (DBT)، والعلاج بالفن ليست سوى عدد قليل من الأساليب المستخدمة. يعمل أطباؤنا السريريون عن كثب مع المرضى لتحديد أنسب العلاجات لاحتياجاتهم الفريدة.
نظام الدعم
يتطلب التعافي من سوء المعاملة نظام دعم قوي. يوفر المركز الألماني لعلم الأعصاب في دبي بيئة آمنة ومراعية حيث يمكن للمرضى مشاركة تجاربهم والتواصل مع الآخرين الذين يواجهون تحديات مماثلة والوصول إلى الموارد اللازمة للتعافي المستمر. يكرس فريقنا المتعاطف جهوده لتمكين الأفراد من إعادة بناء حياتهم.
الخاتمة
إن سوء المعاملة خصم هائل، ولكن مع توفر الموارد والدعم المناسبين، يمكن للضحايا التغلب على قبضته واستعادة السيطرة على حياتهم. يقف المركز الألماني لعلم الأعصاب بدبي كمنارة للأمل، حيث يقدم رعاية شاملة تعالج الجوانب الجسدية والعاطفية والنفسية للإساءة. يلتزم فريقنا المتمرس بتوجيه المرضى نحو طريق الشفاء والتعافي والتمكين. إذا كنت أنت أو أحد أحبائك تسعى للحصول على المساعدة، فتواصل مع المركز الألماني لعلوم الأعصاب بدبي، حيث تتلاقى الرحمة والخبرة لتمهيد الطريق لمستقبل أكثر إشراقاً.
اضطرابات التكيف
المرض
اضطرابات التكيف
اضطراب التكيف يعني أن رد الفعل الطبيعي للتوتر يبدأ بعد شهر من الحدث ويستمر حتى ستة أشهر. سيظل هذا يعتبر رد فعل طبيعي على الرغم من أنه في هذه الحالات أيضًا قد تكون المساعدة العلاجية ضرورية.
© GNC, German Neuroscience Center Dubai (Neurology, Psychiatry, Psychology, Counseling, Dubai, UAE)
الصدمة
يمكن أن يكون للصدمة، بأشكالها المختلفة، تأثير عميق على الصحة البدنية والعاطفية والنفسية للفرد. سواء كانت ناجمة عن حوادث أو عنف أو غيرها من الأحداث المؤلمة، يمكن أن تؤدي الصدمة إلى مجموعة من الأعراض التي قد تؤثر على جودة حياة الشخص. يقف المركز الألماني لعلم الأعصاب (GNC) في دبي كمنارة للأمل والشفاء، حيث يقدم أحدث العلاجات والرعاية الرحيمة لمساعدة الأفراد على التغلب على الصدمات والشروع في رحلة نحو التعافي.
علامات وأعراض الصدمة النفسية
يمكن أن تظهر الصدمة بعدة طرق، وتختلف الأعراض باختلاف شدة وطبيعة الحدث المؤلم. تشمل العلامات الشائعة للصدمة ما يلي:
- إعادة التجربة: ذكريات الماضي والكوابيس والأفكار المتطفلة حول الحدث المؤلم.
- التجنب: تجنب المحفزات المرتبطة بالصدمة، مما يؤدي إلى الانسحاب من الأشخاص أو الأماكن أو الأنشطة.
- فرط الاستثارة: زيادة اليقظة، والتهيج، وصعوبة التركيز، والاستجابة المفاجئة المبالغ فيها.
- الاضطرابات العاطفية: مشاعر شديدة من الشعور بالذنب والخجل والغضب والحزن التي قد تستمر لفترة طويلة بعد الحدث.
- الأعراض الجسدية: الصداع والشد العضلي والتوتر العضلي والإرهاق واضطراب أنماط النوم.
عوامل خطر الإصابة بالصدمة
يمكن أن تزيد بعض العوامل من قابلية الفرد للتعرض للصدمة. وتشمل عوامل الخطر هذه ما يلي:
- صدمة سابقة: يمكن أن يجعل تاريخ التجارب الصادمة السابقة الأفراد أكثر عرضة للصدمات اللاحقة.
- نقص الدعم: يمكن أن تؤدي محدودية أنظمة الدعم الاجتماعي والعزلة إلى تضخيم تأثير الصدمة.
- المرونة الشخصية: قد يتمتع بعض الأفراد بمرونة أكبر، مما يسمح لهم بالتعامل بفعالية أكبر مع الأحداث المؤلمة.
- التعرض للعنف: يمكن أن يؤدي التعرض المتكرر للعنف، سواء كضحية أو كشاهد، إلى زيادة خطر الإصابة بالصدمة.
- حالات الصحة العقلية الموجودة مسبقاً: قد يكون الأفراد الذين يعانون من القلق أو الاكتئاب أو اضطرابات الصحة العقلية الأخرى الموجودة مسبقاً أكثر عرضة للتأثيرات المرتبطة بالصدمات.
أسباب الصدمة وتشخيصها
يمكن أن تنشأ الصدمة من مجموعة من الأحداث، مثل الحوادث والكوارث الطبيعية والعنف بين الأشخاص والإجراءات الطبية. ينطوي تشخيص الصدمة على تقييم شامل يأخذ بعين الاعتبار تاريخ المريض وأعراضه واستجاباته العاطفية. ويستخدم الأطباء المتمرسون في مركز GNC أحدث تقنيات التشخيص، بما في ذلك التقييمات النفسية والتصوير العصبي، لتقييم تأثير الصدمة على الصحة النفسية والجسدية للفرد بدقة.
علاج الصدمات في المركز الألماني لعلوم الأعصاب بدبي
يشتهر المركز الألماني لعلم الأعصاب في دبي بنهجه الشامل في علاج الصدمات، حيث يقدم مجموعة واسعة من التدخلات القائمة على الأدلة والمصممة خصيصاً لتلبية الاحتياجات الفريدة لكل مريض. ويشمل ذلك:
- العلاج النفسي: علاجات فردية وجماعية مثل العلاج السلوكي المعرفي (CBT) وإزالة حساسية حركة العين وإعادة المعالجة (EMDR) لمعالجة الأعراض المرتبطة بالصدمة وتعزيز الشفاء.
- الأدوية: في الحالات التي تكون فيها الأعراض شديدة، يمكن وصف الأدوية المستهدفة للتخفيف من القلق والاكتئاب والأعراض المؤلمة الأخرى.
- تقنيات العقل والجسم: يمكن لممارسات مثل اليوغا والتأمل والتنفس العميق أن تساعد في تنظيم استجابة الجسم للضغط النفسي وتعزيز الصحة النفسية.
- الارتجاع العصبي: تهدف تقنيات الارتجاع العصبي المتطورة إلى إعادة تدريب أنماط الدماغ، مما يسهل التنظيم العاطفي والحد من الأعراض.
- الفن والعلاجات التعبيرية: يمكن للمنافذ الإبداعية أن توفر وسيلة لمعالجة الصدمة عندما تقصر الكلمات.
لماذا تختار المركز الألماني لعلوم الأعصاب دبي؟
يمثل المركز الألماني لعلوم الأعصاب بدبي منارة للأمل والشفاء للأفراد الذين يسعون إلى علاج شامل للصدمات النفسية. وبفضل فريق من الخبراء المشهورين دولياً وأدوات التشخيص المتقدمة والنهج الذي يركز على المريض، يوفر المركز الألماني لعلوم الأعصاب بيئة آمنة وداعمة لمن هم في رحلة التعافي. إن التزام المركز بالتميز والابتكار والرعاية الشخصية هو ما يميزه كوجهة رائدة لعلاج الصدمات في المنطقة.
الخاتمة
يمكن أن تكون آثار الصدمة بعيدة المدى وتؤثر على كل جانب من جوانب حياة الفرد. ولكن مع الرعاية الشاملة والرحيمة التي يقدمها المركز الألماني لعلوم الأعصاب بدبي، فإن الشفاء في متناول اليد. من العلاجات المتطورة إلى الالتزام برفاهية المريض، يمثل المركز الألماني لعلم الأعصاب دبي منارة للأمل يوجه الأفراد نحو مستقبل أكثر إشراقاً حيث يمكن تخفيف قبضة الصدمة واستعادة مباهج الحياة مرة أخرى
اضطراب الأشكال الجسدية
اضطرابات الأشكال الجسدية

تُعرَّف الاضطرابات الجسدية بأنها أعراض جسدية (جسدية) دون وجود سبب جسدي (جسدي) كافٍ. ولا يمكن أخذ العوامل النفسية في الاعتبار إلا بعد استبعاد الأسباب الجسدية. عرض الأعراض هو نفسه، بغض النظر عما إذا كانت ناجمة عن عوامل جسدية أو نفسية. ومن الأمثلة الجيدة على ذلك آلام الظهر الشائعة. يمكن أن يكون سببه انضغاط العصب كسبب جسدي. ويمكن أن يكون الألم نفسه ناتجاً عن عوامل نفسية أيضاً. يبدو هذا الأمر صعب التصديق بالنسبة لمعظم الناس. ومع ذلك، تعد الاضطرابات الجسدية من بين الاضطرابات النفسية الأكثر شيوعًا وتحدث لدى 10 إلى 15% من مرضى الرعاية الأولية.
يمكن أن تسبب اضطرابات الأشكال الجسدية جميع أنواع الأعراض تقريباً. من الألم على متلازمة القولون العصبي حتى الخوف من ورم في المخ. ونظراً لأنه من الطبيعي جداً الاعتقاد بوجود سبب جسدي ما، فإن المرضى يخضعون في خيمة المرضى لفحوصات طبية مختلفة - حتى العمليات الجراحية غير الضرورية. في بعض الأحيان يبحث المرضى عن سبب يفسر الأعراض لسنوات. وهم يستشيرون الأطباء بشكل متكرر، وهو ما يسمى "التنقل بين الأطباء" وغالباً ما يلجأون إلى الطب البديل. يعبر هذا النوع من السلوك عن الضغط الهائل الذي يتعرض له هؤلاء المرضى.
من المهم أن نفهم أن هؤلاء المرضى يعانون من المرض، وسيعانون من آلام واضطرابات وظيفية أو ما شابه ذلك. لا يتظاهر الأشخاص المصابون باضطرابات الأشكال الجسدية بأعراضهم ويمكن أن تؤثر أعراضهم بشكل كبير على أدائهم اليومي. وغالباً ما يكون لألمهم تأثير كبير على العمل والعلاقات والأنشطة الأخرى.
الأنواع والأعراض
1. اضطراب الجسدية / اضطراب الأعراض الجسدية
يتضمن هذا النوع من الاضطراب الجسدي أعراضاً مثل الألم، والمشاكل العصبية، والمشاكل الجنسية، والشكاوى المتعلقة بأمراض النساء والقلب والجهاز الهضمي. وغالباً ما يكون لدى المرضى تاريخ طويل من المشاكل الطبية ولكن لا يوجد تشخيص يمكن أن يفسر جميع أعراضهم.
2. اضطراب الشكل الجسدي غير المتمايز
يتحدث المرء عن اضطراب الشكل الجسدي غير المتمايز إذا كان المريض يعاني من شكوى جسدية واحدة أو أكثر من الأعراض غير المبررة لمدة ستة أشهر على الأقل.
3. الوسواس القهري
إذا كان المريض يشعر بالقلق من وجود مرض خطير ويعتقد أن الشكاوى البسيطة هي علامات على وجود مشاكل طبية خطيرة للغاية فهو يعاني من هذا النوع من الاضطرابات الجسدية.
4. اضطراب التحويل
في هذا النوع، يعاني المريض من أعراض عصبية مثل الشلل أو العمى أو فقدان السمع أو فقدان الإحساس أو التنميل دون أي سبب طبي.
5. اضطراب الألم
يعاني المرضى المصابون باضطراب الألم عادةً من ألم بدأ مع ضغط نفسي أو صدمة نفسية مثل الصداع المزمن بعد حدث حياتي مرهق.
التشخيص
قد يكون العثور على التشخيص صعباً ويستغرق وقتاً طويلاً. هناك حاجة إلى إجراء فحص طبي شامل بما في ذلك الفحوصات المخبرية والفحوصات الإشعاعية لتحديد الأسباب المحتملة للأعراض. من المهم جداً عدم التغاضي عن أي سبب جسدي (جسدي). على الجانب الآخر يجب حماية المريض من الفحوصات الطبية والعمليات الجراحية غير الضرورية. إذا لم يكشف الفحص عن مصدر واضح للألم يمكن النظر في اضطراب جسدي.
إذا كنت غير قادر على معرفة ما هي مشكلتك النفسية، فيمكننا مساعدتك في ذلك بمساعدة أفضل أطباء الأعصاب والطب النفسي وأطباء علم النفس.
العلاج
تلعب العلاقة القوية بين الطبيب والمريض دوراً رئيسياً في العلاج الفعال لاضطرابات الشكل الجسدي. بالنسبة للمريض، من المهم أن يفهم أن علاج اضطراب الشكل الجسدي لا يعني إهمال احتمال وجود سبب جسدي. فهو ليس قرارًا إما أن يتخذ المريض قرارًا أو لا. بل إن علاج اضطراب الشكل الجسدي بشكل صحيح هو إضافة إلى المحاولات التي قام بها المريض حتى الآن. سيقوم الطبيب بتقييم جميع الإجراءات التي تم إجراؤها ويقرر مع المريض أي الفحوصات الإضافية ضرورية وأيها غير ضرورية. سيضع المريض والطبيب معاً تصوراً يأخذ جميع العوامل المؤثرة على المرض في الاعتبار. يمكن أن تكون هذه العوامل مختلفة جداً من مريض لآخر. وبناءً على ذلك، تكون أشكال العلاج المختلفة فعالة. يتم استخدام العلاج السلوكي المعرفي لأنه يركز على تصحيح الأفكار المشوهة والمعتقدات والسلوكيات غير الواقعية التي تحفز القلق الصحي. ينصب التركيز بدلاً من ذلك على تحسين الأداء اليومي ثم على إدارة الأعراض. وغالبًا ما يكون الحد من التوتر جزءًا مهمًا من التحسن. يمكن أن تدعم الأدوية المضادة للاكتئاب العلاج النفسي. علاوة على ذلك، يمكن أن تكون مجموعات الدعم مفيدة وكذلك تمارين الحد من التوتر والعلاج الطبيعي والتدليك. سيضع الطبيب خطة علاج فردية لكل مريض.
اضطراب الوسواس القهري (OCD)
اضطراب الوسواس القهري (OCD) هو حالة صحية نفسية معقدة تؤثر على ملايين الأشخاص في جميع أنحاء العالم. يتسم الوسواس القهري بالأفكار المستمرة والمزعجة (الوساوس) والسلوكيات المتكررة (القهرية)، ويمكن أن يعرقل الوسواس القهري حياة الفرد اليومية بشكل كبير، مما يسبب له الضيق والقلق. إذا كنت تعاني أنت أو أحد أحبائك من اضطراب الوسواس القهري، فكن مطمئنًا أن المركز الألماني لعلم الأعصاب في دبي مكرس لتقديم رعاية شاملة ومتخصصة لمساعدتك في التغلب على هذه التحديات.
أعراض اضطراب الوسواس القهري (OCD)
يتجلى الوسواس القهري من خلال مجموعة واسعة من الأعراض، وغالبًا ما ينطوي على أفكار متطفلة والحاجة إلى القيام بسلوكيات معينة للتخفيف من القلق. تشمل الوساوس الشائعة الخوف من التلوث، والمخاوف من إيذاء النفس أو الآخرين، والحاجة الملحة إلى التناسق والنظام. من ناحية أخرى، قد تنطوي الوساوس القهرية على أفعال متكررة مثل غسل اليدين أو فحص الأقفال أو عدّ الأشياء لتخفيف الضيق الناجم عن الوساوس.
عوامل خطر الإصابة باضطراب الوسواس القهري (OCD)
في حين أن السبب الدقيق للوسواس القهري لا يزال غير واضح، فقد تم تحديد العديد من عوامل الخطر:
- الوراثة: يمكن أن يزيد التاريخ العائلي للوسواس القهري من احتمالية الإصابة بالاضطراب.
- بنية الدماغ ووظيفته: قد تساهم بعض التشوهات الدماغية أو الاختلالات في الناقلات العصبية في الإصابة بالوسواس القهري.
- الصدمة: يمكن أن تؤدي صدمة الطفولة أو الضغوطات الحياتية الكبيرة إلى ظهور الوسواس القهري لدى الأفراد المعرضين للإصابة به.
- سمات الشخصية: الكمالية، ومستويات عالية من القلق، والميل إلى القلق المفرط يمكن أن يزيد من الضعف.
أسباب اضطراب الوسواس القهري (OCD)
من المحتمل أن يتأثر تطور الوسواس القهري بمزيج من العوامل الوراثية والعصبية والبيئية. تشير الأبحاث إلى أن التفاعل بين الاستعداد الوراثي وكيمياء الدماغ يلعب دوراً حاسماً. يُعتقد أن التشوهات في دوائر الدماغ التي تشمل العقد القاعدية والقشرة الأمامية تساهم في ظهور أعراض الاضطراب.
تشخيص اضطراب الوسواس القهري (OCD)
ينطوي تشخيص الوسواس القهري على إجراء تقييم شامل لأعراض الفرد وتأثيرها على أدائه اليومي. سيُجري أخصائي الصحة النفسية الماهر في المركز الألماني لعلوم الأعصاب في دبي تقييماً شاملاً قد يتضمن مقابلات واستبيانات نفسية ومناقشات حول تاريخ الأعراض ومدتها. تضمن هذه العملية الدقيقة تشخيصاً دقيقاً وخطة علاجية مخصصة.
علاجات اضطراب الوسواس القهري (OCD)
غالبًا ما تتطلب الإدارة الفعالة للوسواس القهري مزيجًا من العلاج والأدوية. يمكن للطبيب النفسي في دبي أن يصمم خطة علاجية تتضمن العلاج السلوكي المعرفي والأدوية والتقنيات المتقدمة مثل التحفيز المغناطيسي المتكرر عبر الجمجمة. في المركز الألماني لعلم الأعصاب في دبي، يتم استخدام نهج متعدد التخصصات لتوفير أكثر العلاجات فعالية للوسواس القهري:
- العلاج المعرفي السلوكي المعرفي (CBT): يُعد العلاج المعرفي السلوكي، وخاصةً العلاج المعرفي السلوكي المعرفي (ERP)، علاجًا نفسيًا قياسيًا ذهبيًا للوسواس القهري. وهو ينطوي على التعرض التدريجي للمواقف أو الأفكار المخيفة وتعلم طرق أكثر صحة لإدارة القلق دون اللجوء إلى الإكراه.
- الأدوية: توصف عادةً مثبطات امتصاص السيروتونين الانتقائية (SSRIs) لعلاج أعراض الوسواس القهري. تساعد هذه الأدوية على تنظيم مستويات الناقلات العصبية في الدماغ ويمكن أن تكون مفيدة بشكل خاص عندما تقترن بالعلاج.
- التحفيز المغناطيسي العميق عبر الجمجمة (dTMS): يستخدم هذا الإجراء المبتكر غير الجراحي مجالات مغناطيسية لتحفيز مناطق معينة في الدماغ، مما يساعد على تعديل الدوائر العصبية المرتبطة بأعراض الوسواس القهري.
- مجموعات الدعم والتثقيف: يمكن أن يساعد الانخراط في مجموعات الدعم وتلقي التثقيف حول الوسواس القهري الأفراد وعائلاتهم على فهم الاضطراب بشكل أفضل والتأقلم معه بفعالية.
لماذا تختار مركز علم الأعصاب الألماني دبي لعلاج الوسواس القهري
يبرز المركز الألماني لعلوم الأعصاب بدبي كمؤسسة رائدة في علاج الوسواس القهري نظراً لالتزامه بتقديم رعاية تتمحور حول المريض:
- الخبرة: يضم المركز فريقاً من الأطباء النفسيين والأخصائيين النفسيين والمعالجين النفسيين ذوي الخبرة والفهم العميق للوسواس القهري وتعقيداته.
- خطط علاج مصممة خصيصاً: يتلقى كل مريض خطة علاجية مخصصة بناءً على احتياجاته وتفضيلاته الفريدة، مما يضمن أعلى فرص للنجاح.
- العلاجات المتطورة: يقدم المركز مجموعة واسعة من العلاجات القائمة على الأدلة، بما في ذلك العلاج السلوكي المعرفي السلوكي والأدوية والعلاجات المتقدمة مثل التحفيز المغناطيسي المتكرر عبر الجمجمة.
- النهج الشمولي: يدرك فريق العمل في المركز الألماني لعلوم الأعصاب بدبي أهمية معالجة الجوانب النفسية والعاطفية للوسواس القهري وتعزيز الرفاهية بشكل عام.
الخاتمة
يمكن أن يكون اضطراب الوسواس القهري حالة يصعب التعامل معها، ولكن مع الدعم والعلاج المناسبين، يمكن للأفراد استعادة السيطرة على حياتهم. يكرس المركز الألماني لعلم الأعصاب في دبي جهوده لتوفير أعلى مستوى من الرعاية للأفراد الذين يعانون من اضطراب الوسواس القهري. ومن خلال مزيج من المعرفة المتخصصة وخطط العلاج المخصصة والعلاجات المتقدمة، يلتزم المركز بمساعدة المرضى على التغلب على سيطرة الوسواس القهري والتمتع بحياة أكثر صحة وإشباعاً.
الاضطراب الانفصامي (التحويلات)
المرض
الاضطراب الانفصامي (التحويلات)
تعريف الاضطراب الفصامي
يمكن أن تؤدي الأحداث المؤلمة أو المشاكل التي تبدو غير قابلة للحل إلى رد فعل نفسي يُعرف بالاضطراب الانفصامي. ويتميز هذا الاضطراب بالانفصال وعدم الاستمرارية بين الأفكار والذكريات والمحيط والأفعال والهوية. يشعر الأشخاص المصابون بالاضطراب الانفصامي بأن أجسادهم أو العالم من حولهم غير حقيقيين وهم غير متأكدين من هويتهم. قد يشعرون بأن لديهم العديد من الهويات المختلفة مما يؤدي في كثير من الأحيان إلى مشاكل في الأداء في الحياة اليومية. وقد يهربون من الواقع بطرق لا إرادية وغير صحية.
الأعراض
يمكن أن تشمل علامات وأعراض الاضطراب الانفصامي فقدان الذاكرة (فقدان الذاكرة) لفترات زمنية معينة وأحداث وأشخاص معينين، وعدم القدرة على تذكر المعلومات الشخصية الرئيسية التي لا يمكن تفسيرها على أنها مجرد نسيان، والشعور بالانفصال عن الذات وعدم وضوح الإحساس بالهوية. إلى جانب الانفصام وتعدد الشخصيات أو انفصام الشخصية قد يعاني الأشخاص أيضًا من الاكتئاب وتقلب المزاج واضطراب النوم والقلق ونوبات الهلع واضطرابات الأكل وغيرها.
ينقسم الاضطراب الانفصالي إلى ثلاثة اضطرابات رئيسية:
- فقدان الذاكرة الانفصامي: يحجب الأشخاص الذين يعانون من هذا الاضطراب المعلومات الشخصية المهمة، وعادةً ما تكون ذات طبيعة صادمة أو مرهقة. فهم لا يستطيعون تذكر معلومات عن أنفسهم أو الأحداث والأشخاص في حياتهم، خاصةً من فترة مؤلمة. تكون هذه الفجوات في الذاكرة أكثر حدة من النسيان العادي، وهي ليست نتيجة لحالة طبية كامنة.
- اضطراب الهوية الانفصامية: يتسم هذا الاضطراب بالهويات البديلة. قد يشعر الأشخاص بوجود شخص آخر أو أكثر يتحدثون أو يعيشون داخل رؤوسهم ويشعرون كما لو كانوا ممسوسين بهويات أخرى. كان هذا الاضطراب يُعرف سابقًا باسم اضطراب تعدد الشخصيات وهو أشهر الاضطرابات الانفصامية. وعادةً ما يعاني الأشخاص المصابون باضطراب الهوية الانفصامية أيضًا من فقدان الذاكرة الانفصامي وغالبًا ما يكون لديهم شرود فصامي.
- اضطراب تبدد الشخصية-تبدد الإحساس بالذات: يعاني الأشخاص المصابون بهذا الاضطراب من شعور بأنهم خارج أنفسهم. فهم يراقبون أفعالهم ومشاعرهم وأفكارهم من مسافة بعيدة كما لو كانوا يشاهدون فيلمًا. ويعاني الشخص المصاب باضطراب تبدد الشخصية من هذه التجربة بشكل متكرر وشديد لدرجة أنها تعيق أداءه وخبراته.
الأسباب
تتمثل الأسباب الرئيسية للاضطراب الانفصالي في الأحداث الصادمة في الماضي مثل الإيذاء الجسدي أو الجنسي أو العاطفي الذي تعرض له الشخص أثناء الطفولة، على الرغم من أن بعض الأشخاص "ينفصلون" بعد التعرض للحرب أو الاختطاف أو حتى إجراء طبي جائر. يعد الانعزال عن الواقع آلية دفاعية طبيعية للتكيف خلال فترة الصدمة ولكنها تصبح مختلة عندما لا تكون البيئة التي تعرض لها الشخص صادمة ولكنه لا يزال يتصرف ويعيش كما لو كانت كذلك.
العلاج
العلاج الأساسي للاضطراب الانفصامي هو العلاج النفسي. ستساعد استشارة المعالج النفسي المريض على فهم سبب الحالة وتكوين طرق جديدة للتعامل مع الظروف المجهدة. قد يستفيد الشخص المصاب بالاضطراب الفصامي أيضًا من الأدوية مثل مضادات الاكتئاب أو الأدوية المضادة للقلق. يمكن أن تساعد هذه الأدوية في السيطرة على أعراض الصحة العقلية المرتبطة بالاضطرابات الانفصامية.
© GNC, German Neuroscience Center Dubai (Neurology, Psychiatry, Psychology, Counseling, Dubai, UAE)









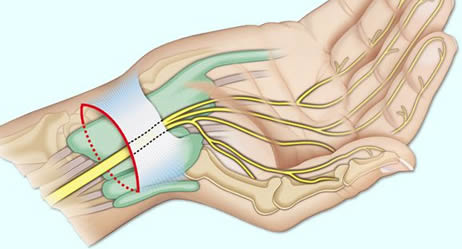




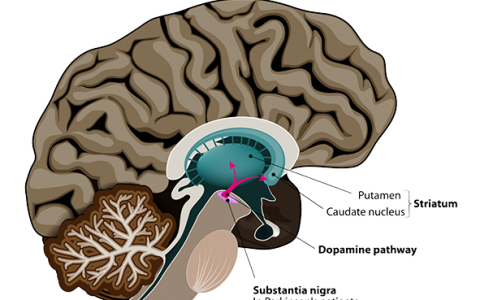



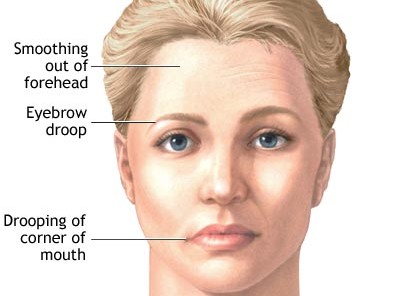



























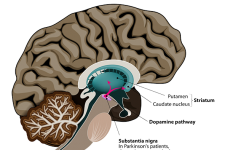



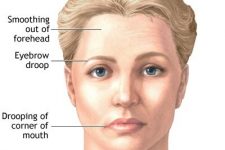













Tالمركز الألماني للعلوم العصبية يعرض مجموعة مختارة من الأمراض العصبية والنفسية الشائعة. في الأعلى سوف تجد زرا حيث يمكنك الإختيار ما بين الأمراض العصبية و النفسية الأمراض النفسية . بالضغط هنا يمكنك اختيار ما بين الأمراض العصبية والنفسية . بالضغط على الصورة يمكنك يمكنك التعرف على المزيد من المعلومات عن المرض كالسكتات الدماغية والصرع والتصلب المتعدد والشلل الرعاش وإعتلال الأعصاب و آلام الظهر وتلف الأعصاب و متلازمة النفق الرسغي و الصداع النصفي و الدوار و الوهن العضلي والشلل و متلازمة تملل الساقين والرعاش، و التهاب العصب الثالث ، و الإضطرابات البصرية ، والخرف ، والفصام ، والاكتئاب ، والهوس ، و ثنائي القطب ، وهجمات الهلع و القلق و الخوف ، والوسواس القهري ،و الإضطرابات النفسية الحادة ، و اضطراب ما بعد الصدمة ، واضطرابات التكيف، و الإضطراب الجسدي ، و الإضطراب الفصامي ، و اضطرابات الطعام ، و اضطراب النوم ، و اضطراب نقص الانتباه و النشاط المفرط والتوحد مع خيارات العلاج في دبي.
© المركز الألماني للأمراض العصبية و النفسية في دبي (طب الأعصاب الطب النفسي علم النفس في دبي)
German Neuroscience Center © Copyright
